

Limits of normality of quantitative thoracic CT analysis
- PMID: 23706034
- PMCID: PMC4057220
- DOI: 10.1186/cc12738
Limits of normality of quantitative thoracic CT analysis
Abstract
Introduction: Although computed tomography (CT) is widely used to investigate different pathologies, quantitative data from normal populations are scarce. Reference values may be useful to estimate the anatomical or physiological changes induced by various diseases.
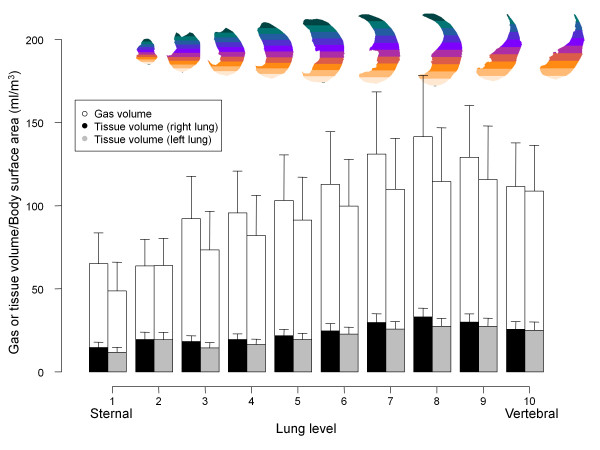
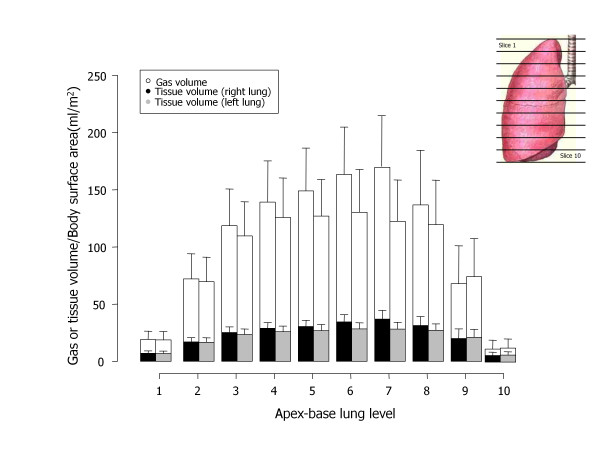
Methods: We analyzed 100 helical CT scans taken for clinical purposes and referred as nonpathological by the radiologist. Profiles were manually outlined on each CT scan slice and each voxel was classified according to its gas/tissue ratio. For regional analysis, the lungs were divided into 10 sterno-vertebral levels.
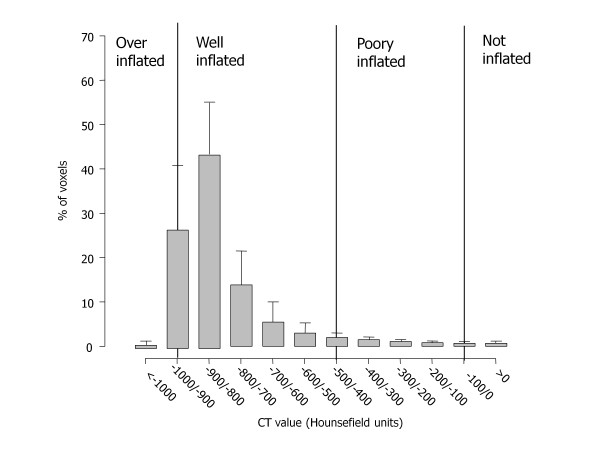
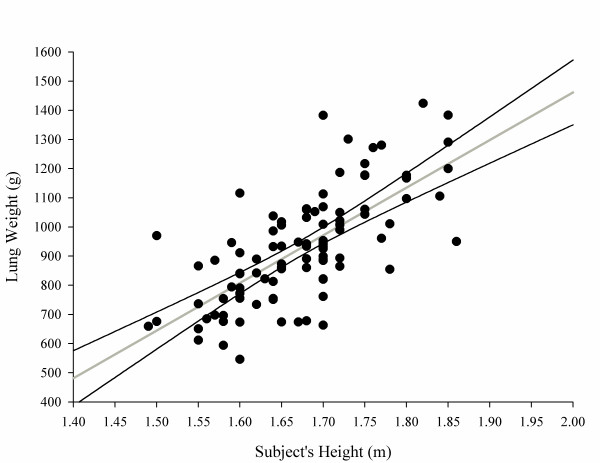
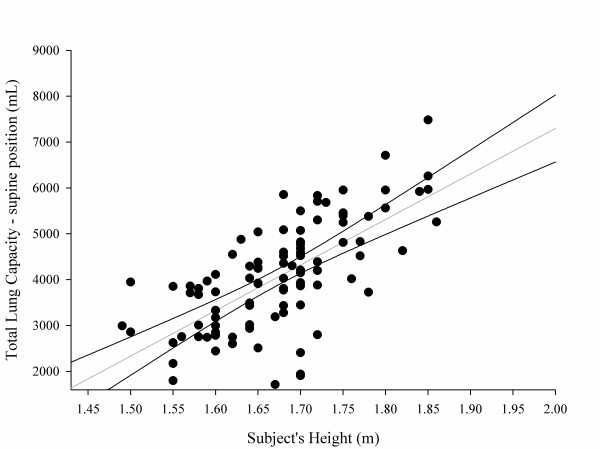
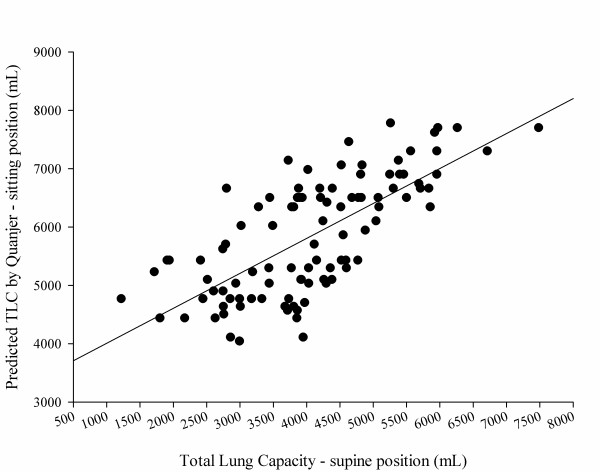
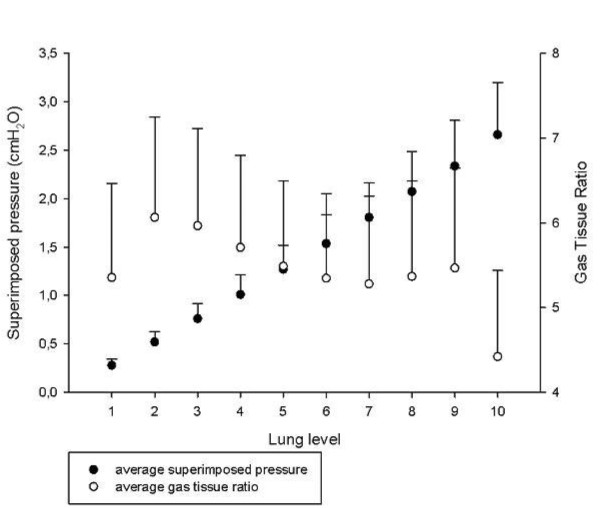
Results: We studied 53 males and 47 females (age 64 ± 13 years); males had a greater total lung volume, lung gas volume and lung tissue. Noninflated tissue averaged 7 ± 4% of the total lung weight, poorly inflated tissue averaged 18 ± 3%, normally inflated tissue averaged 65 ± 8% and overinflated tissue averaged 11 ± 7%. We found a significant correlation between lung weight and subject's height (P <0.0001, r2 = 0.49); the total lung capacity in a supine position was 4,066 ± 1,190 ml, ~1,800 ml less than the predicted total lung capacity in a sitting position. Superimposed pressure averaged 2.6 ± 0.5 cmH2O.
Conclusion: Subjects without lung disease present significant amounts of poorly inflated and overinflated tissue. Normal lung weight can be predicted from patient's height with reasonable confidence.
Figures
References
-
- Gattinoni L, Chiumello D, Cressoni M. Pulmonary computed tomography and adult respiratory distress syndrome. Swiss Med Wkly. 2005;17:169–174. - PubMed
-
- Gattinoni L, Pesenti A, Bombino M. Relationships between lung computed tomographic density, gas exchange, and PEEP in acute respiratory failure. Anesthesiology. 1988;17:824–832. - PubMed
-
- Gattinoni L, Bombino M, Pelosi P. Lung structure and function in different stages of severe adult respiratory distress syndrome. JAMA. 1994;17:1772–1779. - PubMed
-
- Gattinoni L, D'Andrea L, Pelosi P. Regional effects and mechanism of positive end-expiratory pressure in early adult respiratory distress syndrome. JAMA. 1993;17:2122–2127. - PubMed
-
- Gattinoni L, Pelosi P, Vitali G, Pesenti A, D'Andrea L, Mascheroni D. Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure. Anesthesiology. 1991;17:15–23. - PubMed
