

Treatment of acute visceral aortic pathology with fenestrated/branched endovascular repair in high-surgical-risk patients
- PMID: 23706619
- PMCID: PMC4183351
- DOI: 10.1016/j.jvs.2012.12.043
Treatment of acute visceral aortic pathology with fenestrated/branched endovascular repair in high-surgical-risk patients
Abstract
Objective: The safety and feasibility of fenestrated/branched endovascular repair of acute visceral aortic disease in high-risk patients is unknown. The purpose of this report is to describe our experience with surgeon-modified endovascular aneurysm repair (sm-EVAR) for the urgent or emergent treatment of pathology involving the branched segment of the aorta in patients deemed to have prohibitively high medical and/or anatomic risk for open repair.
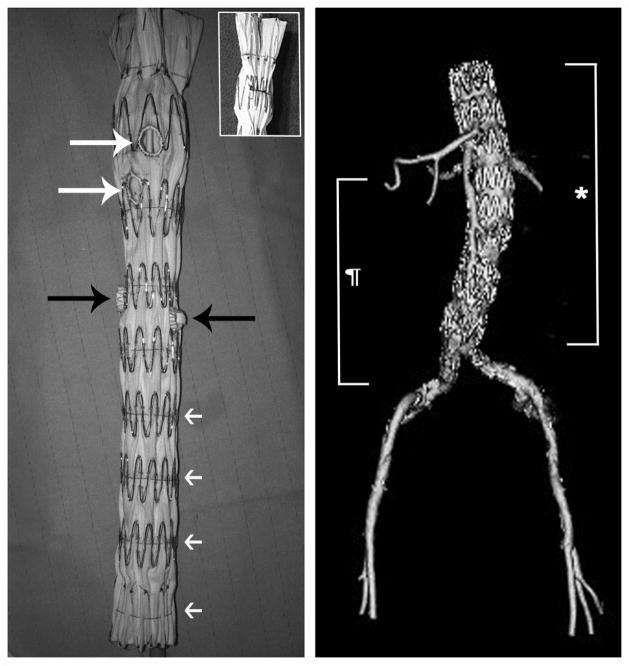
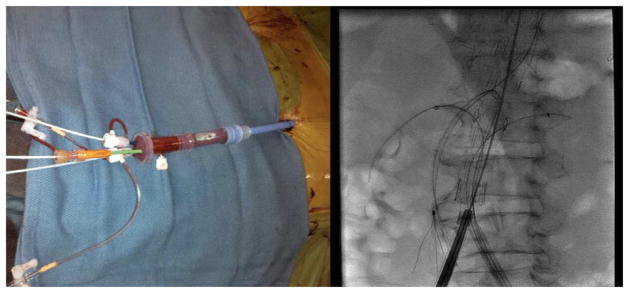
Methods: A retrospective review was performed on all patients treated with sm-EVAR for acute indications. Planning was based on three-dimensional computed tomographic angiogram reconstructions and graft configurations included various combinations of branch, fenestration, or scallop modifications.
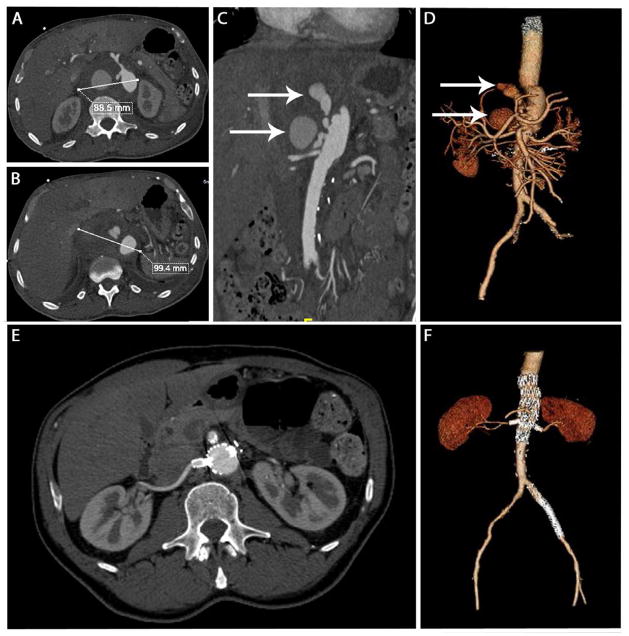
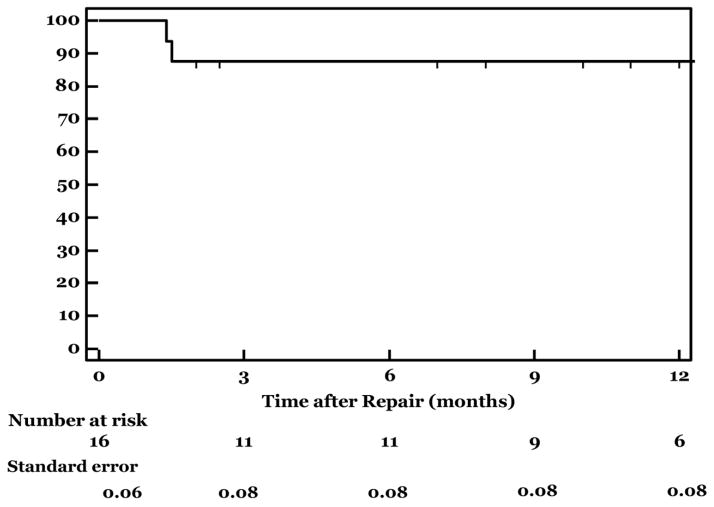
Results: Sixteen patients (mean age [± standard deviation], 68 ± 10 years; 88% male) deemed high risk for open repair underwent urgent or emergent repair using sm-EVAR. Indications included degenerative suprarenal or thoracoabdominal aneurysm (six), presumed or known mycotic aneurysm (four), anastomotic pseudoaneurysm (three), false lumen rupture of type B dissection (two), and penetrating aortic ulceration (one). Nine (56%) had previous aortic surgery and all patients were either American Society of Anesthesiologists class IV (n = 9) or IV-E (n = 7). A total of 40 visceral vessels (celiac, 10; superior mesenteric artery, 10; right renal artery, 10; left renal artery, 10) were revascularized with a combination of fenestrations (33), directional graft branches (six), and graft scallops (one). Technical success was 94% (n = 15/16), with one open conversion. Median contrast use was 126 mL (range, 41-245) and fluoroscopy time was 70 minutes (range, 18-200). Endoleaks were identified intraoperatively in four patients (type II, n = 3; type IV, n = 1), but none have required remediation. Mean length of stay was 12 ± 15 days (median, 5.5; range, 3-59). Single complications occurred in five (31%) patients as follows: brachial sheath hematoma (one), stroke (one), ileus (one), respiratory failure (one), and renal failure (one). An additional patient experienced multiple complications including spinal cord ischemia (one) and multiorgan failure resulting in death (n = 1; in-hospital mortality, 6.3%). The majority of patients were discharged to home (63%; n = 10) or short-term rehabilitation units (25%; n = 4), while one patient required admission to a long-term acute care setting. There were no reinterventions at a median follow-up of 6.2 (range, 1-16.1) months. Postoperative computed tomographic angiogram was available for all patients and demonstrated 100% branch vessel patency, with one type III endoleak pending intervention. There were two late deaths at 1.4 and 13.4 months due to nonaortic-related pathology.
Conclusions: Urgent or emergent treatment of acute pathology involving the visceral aortic segment with fenestrated/branched endograft repair is feasible and safe in selected high-risk patients; however, the durability of these repairs is yet to be determined.
Copyright © 2013 Society for Vascular Surgery. All rights reserved.
Figures
Similar articles
-
Outcomes of surgeon-modified fenestrated-branched endograft repair for acute aortic pathology.J Vasc Surg. 2015 Nov;62(5):1148-59.e2. doi: 10.1016/j.jvs.2015.06.133. Epub 2015 Aug 5. J Vasc Surg. 2015. PMID: 26254453 Free PMC article.
-
Fenestrated and Branched Endograft after Previous Aortic Repair.Ann Vasc Surg. 2016 Apr;32:119-27. doi: 10.1016/j.avsg.2015.10.018. Epub 2016 Jan 22. Ann Vasc Surg. 2016. PMID: 26806249
-
In situ laser fenestration during emergent thoracic endovascular aortic repair is an effective method for left subclavian artery revascularization.J Vasc Surg. 2013 Nov;58(5):1171-7. doi: 10.1016/j.jvs.2013.04.045. Epub 2013 Jun 5. J Vasc Surg. 2013. PMID: 23746832
-
The Initial Experience on Branched and Fenestrated Endografts in the Aortic Arch. A Systematic Review.Ann Vasc Surg. 2021 Aug;75:29-44. doi: 10.1016/j.avsg.2021.03.024. Epub 2021 Apr 5. Ann Vasc Surg. 2021. PMID: 33831530
-
Systematic review and meta-analysis of published studies on endovascular repair of thoracoabdominal aortic aneurysms with the t-Branch off-the-shelf multibranched endograft.J Vasc Surg. 2020 Aug;72(2):716-725.e1. doi: 10.1016/j.jvs.2020.01.049. Epub 2020 Apr 1. J Vasc Surg. 2020. PMID: 32247700
Cited by
-
Presentation and Outcomes of Elective and Nonelective Complex Endovascular Repair for Thoracoabdominal and Juxtarenal Aortic Aneurysms.Ann Vasc Surg. 2023 Nov;97:248-256. doi: 10.1016/j.avsg.2023.09.001. Epub 2023 Sep 14. Ann Vasc Surg. 2023. PMID: 37714262 Free PMC article.
-
Outcomes of surgeon-modified fenestrated-branched endograft repair for acute aortic pathology.J Vasc Surg. 2015 Nov;62(5):1148-59.e2. doi: 10.1016/j.jvs.2015.06.133. Epub 2015 Aug 5. J Vasc Surg. 2015. PMID: 26254453 Free PMC article.
-
Physician-Modified Endografts for Repair of Complex Abdominal Aortic Aneurysms: Clinical Perspectives and Medico-Legal Profiles.J Pers Med. 2024 Jul 17;14(7):759. doi: 10.3390/jpm14070759. J Pers Med. 2024. PMID: 39064014 Free PMC article. Review.
-
Acute bilateral renal artery chimney stent thrombosis after endovascular repair of a juxtarenal abdominal aortic aneurysm.J Vasc Surg. 2015 Apr;61(4):1058-61. doi: 10.1016/j.jvs.2013.10.037. Epub 2013 Nov 16. J Vasc Surg. 2015. PMID: 24246538 Free PMC article.
-
Three-dimensional fusion computed tomography decreases radiation exposure, procedure time, and contrast use during fenestrated endovascular aortic repair.J Vasc Surg. 2015 Feb;61(2):309-16. doi: 10.1016/j.jvs.2014.07.097. Epub 2014 Aug 28. J Vasc Surg. 2015. PMID: 25175634 Free PMC article.
References
-
- Resch TA, Sonesson B, Dias N, Malina M. Chimney grafts: Is there a need and will they work? Perspect Vasc Surg Endovasc Ther. 2011;23:149–153. - PubMed
-
- Pecoraro F, Pfammatter T, Mayer D, Frauenfelder T, Papadimitriou D, Hechelhammer L, Veith FJ, Lachat M, Rancic Z. Multiple periscope and chimney grafts to treat ruptured thoracoabdominal and pararenal aortic aneurysms. J Endovasc Ther. 2011;18:642–649. - PubMed
-
- Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Experience with 1509 patients undergoing thoracoabdominal aortic operations. J Vasc Surg. 1993;17:357–368. discussion 368–370. - PubMed
-
- Coselli JS. Thoracoabdominal aortic aneurysms: Experience with 372 patients. J Card Surg. 1994;9:638–647. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
