

Fluorescein angiography versus optical coherence tomography for diagnosis of uveitic macular edema
- PMID: 23706700
- PMCID: PMC3758459
- DOI: 10.1016/j.ophtha.2013.01.069
Fluorescein angiography versus optical coherence tomography for diagnosis of uveitic macular edema
Abstract
Objective: To evaluate agreement between fluorescein angiography (FA) and optical coherence tomography (OCT) results for diagnosis of macular edema in patients with uveitis.
Design: Multicenter cross-sectional study.
Participants: Four hundred seventy-nine eyes with uveitis from 255 patients.
Methods: The macular status of dilated eyes with intermediate uveitis, posterior uveitis, or panuveitis was assessed via Stratus-3 OCT and FA. To evaluate agreement between the diagnostic approaches, κ statistics were used.
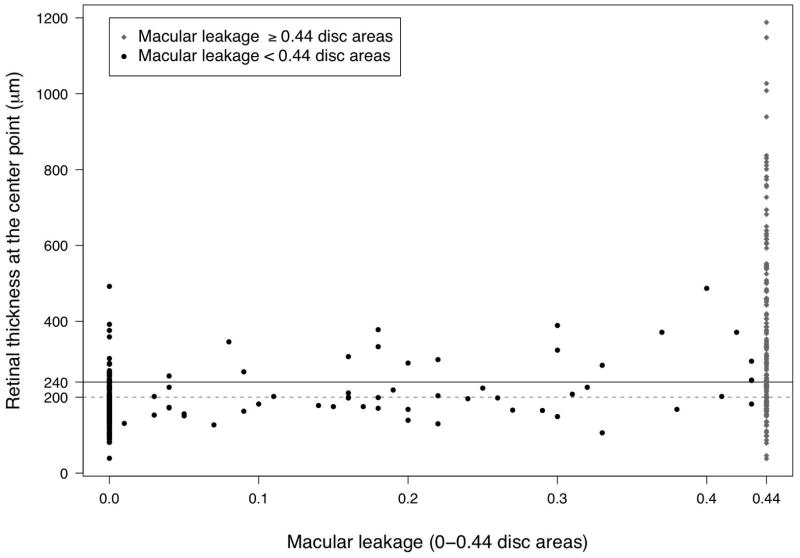
Main outcome measures: Macular thickening (MT; center point thickness, ≥ 240 μm per reading center grading of OCT images) and macular leakage (ML; central subfield fluorescein leakage, ≥ 0.44 disc areas per reading center grading of FA images), and agreement between these outcomes in diagnosing macular edema.
Results: Optical coherence tomography (90.4%) more frequently returned usable information regarding macular edema than FA (77%) or biomicroscopy (76%). Agreement in diagnosis of MT and ML (κ = 0.44) was moderate. Macular leakage was present in 40% of cases free of MT, whereas MT was present in 34% of cases without ML. Biomicroscopic evaluation for macular edema failed to detect 40% and 45% of cases of MT and ML, respectively, and diagnosed 17% and 17% of cases with macular edema that did not have MT or ML, respectively; these results may underestimate biomicroscopic errors (ophthalmologists were not explicitly masked to OCT and FA results). Among eyes free of ML, phakic eyes without cataract rarely (4%) had MT. No factors were found that effectively ruled out ML when MT was absent.
Conclusions: Optical coherence tomography and FA offered only moderate agreement regarding macular edema status in uveitis cases, probably because what they measure (MT and ML) are related but nonidentical macular pathologic characteristics. Given its lower cost, greater safety, and greater likelihood of obtaining usable information, OCT may be the best initial test for evaluation of suspected macular edema. However, given that ML cannot be ruled out if MT is absent and vice versa, obtaining the second test after negative results on the first seems justified when detection of ML or MT would alter management. Given that biomicroscopic evaluation for macular edema erred frequently, ancillary testing for macular edema seems indicated when knowledge of ML or MT status would affect management.
Financial disclosure(s): Proprietary or commercial disclosure may be found after the references.
Copyright © 2013 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Diagnostik des Makulaödems bei Uveitis.Ophthalmologe. 2014 Sep;111(9):814. Ophthalmologe. 2014. PMID: 25343167 German. No abstract available.
References
-
- Durrani OM, Meads CA, Murray PI. Uveitis: a potentially blinding disease. Ophthalmologica. 2004;218:223–36. - PubMed
-
- National Advisory Eye Council. Vision Research. A National Plan, 1983–1987. Chapter 1, Introduction. Bethesda, MD: National Institutes of Health, Public Health Service, US Department of Health and Human Services; 1983. p. 13. Support for Vision Research. vol. 1. NIH Publication 83–2469.
-
- Nussenblatt RB. The natural history of uveitis. Int Ophthalmol. 1990;14:303–8. - PubMed
-
- ten Doesschate J. Causes of blindness in The Netherlands. Doc Ophthalmol. 1982;52:279–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
