

Alternative ankle-brachial index method identifies additional at-risk individuals
- PMID: 23707317
- PMCID: PMC3732795
- DOI: 10.1016/j.jacc.2013.04.061
Alternative ankle-brachial index method identifies additional at-risk individuals
Abstract
Objectives: The aim of this study was to determine whether use of an alternative ankle-brachial index (ABI) calculation method improves mortality risk prediction compared with traditional methods.
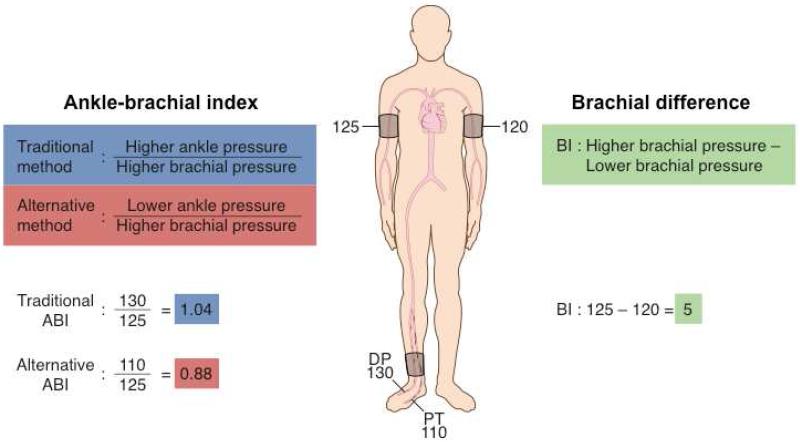
Background: The ABI is used to diagnose peripheral arterial disease (PAD) and to identify those at risk for cardiovascular events. Traditionally, the ABI is calculated with the higher of the dorsalis pedis and posterior tibial ankle arteries. Studies directly comparing calculation methods are limited.
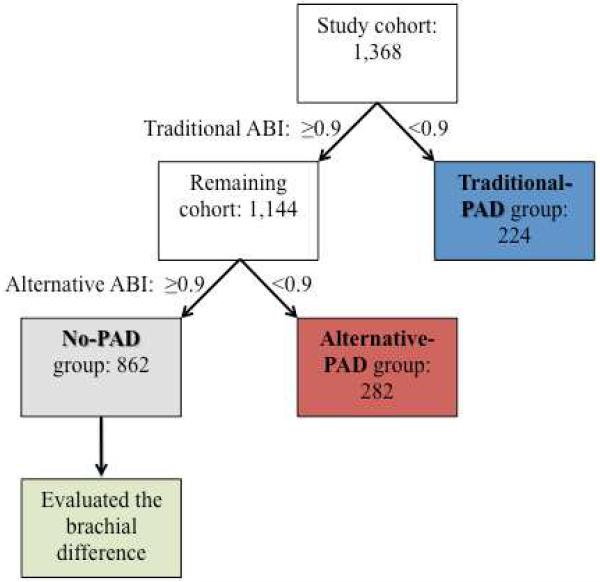
Methods: The ABI was calculated at baseline in 1,413 study participants undergoing non-emergent coronary angiography subsequently followed for all-cause and cardiovascular mortality. There were 224 individuals assigned to the traditional-PAD group (ABI <0.90) with the traditional ABI method. Of those remaining, an alternative ABI method using the lower of the 2 ankle pressures assigned 282 patients to the alternative-PAD group. The 862 individuals not assigned to PAD by either method were the no-PAD group.
Results: There were 163 mortalities during a median follow-up of 5.0 years. Adjusted Cox regression models showed that the alternative-PAD group had an increased risk for all-cause (hazard ratio [HR]: 1.49; 95% confidence interval: 1.01 to 2.19) and cardiovascular mortality (HR: 3.21; 95% confidence interval: 1.53 to 6.37) versus the no-PAD group. Additionally, in the no-PAD group, there was an 11% (HR: 1.11; 95% confidence interval: 1.05 to 1.17) increased risk of all-cause mortality/1-mm Hg increased difference between the left and right brachial systolic pressures.
Conclusions: The implementation of an alternative ABI method and use of the brachial difference identifies individuals at an increased risk for mortality who are currently missed with traditional ABI methods. Current ABI protocols might need to be evaluated.
Keywords: ABI; BMI; CAD; HDL; HR; MACE; ankle-brachial index; body mass index; coronary artery disease; diagnosis; hazard ratio; high-density lipoprotein; major adverse cardiovascular event(s); mortality; peripheral artery disease.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Should an alternate ABI definition be adopted to evaluate risk?J Am Coll Cardiol. 2013 Aug 6;62(6):560-1. doi: 10.1016/j.jacc.2013.04.056. Epub 2013 May 22. J Am Coll Cardiol. 2013. PMID: 23707314 No abstract available.
References
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation. 2004;110:738–43. - PubMed
-
- Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286:1317–24. - PubMed
-
- Newman AB, Shemanski L, Manolio TA. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. The Cardiovascular Health Study Group. Arterioscler Thromb Vasc Biol. 1999;19:538–45. - PubMed
-
- Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med. 1992;326:381–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
