

Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors
- PMID: 23708166
- PMCID: PMC3695631
- DOI: 10.1016/j.ahj.2013.03.020
Atrial fibrillation among Medicare beneficiaries hospitalized with sepsis: incidence and risk factors
Abstract
Background: Newly diagnosed atrial fibrillation (AF) during severe sepsis is associated with increased risks of in-hospital stroke and mortality. However, the prevalence, incidence, and risk factors associated with AF during the sepsis syndromes are unclear.
Methods: We identified patients with preexisting, newly diagnosed, or no AF in a nationally representative 5% sample of Medicare beneficiaries hospitalized with sepsis between 2004 and 2007. We identified multivariable-adjusted demographic and clinical characteristics associated with development of newly diagnosed AF during a sepsis hospitalization.
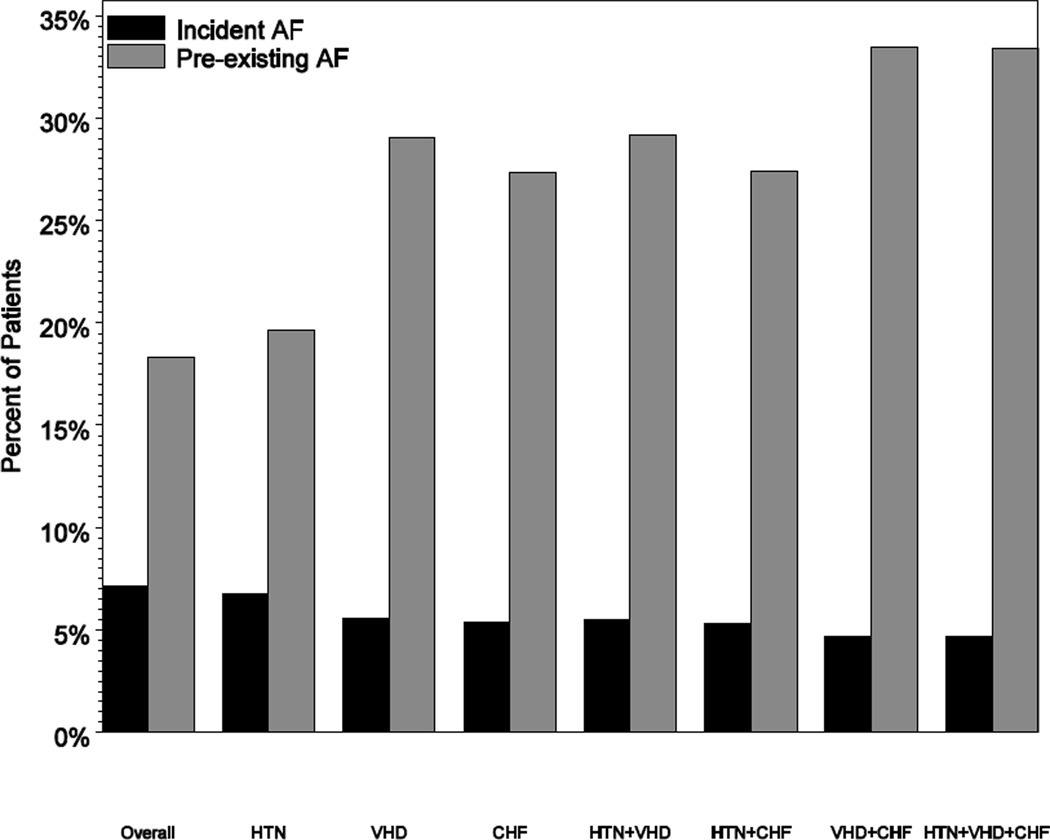
Results: A total of 60,209 beneficiaries had a sepsis hospitalization. Mean age was 80.2 years, 44.4% were men, and 83.1% were white. Atrial fibrillation occurred during 25.5% (95% CI 25.2-25.9) of sepsis hospitalizations, including 18.3% (18.0%-18.7%) with preexisting AF and 7.2% (7.0%-7.4%) with newly diagnosed AF. Patients with sepsis requiring intensive care had a greater risk of newly diagnosed AF (10.7%, 95% CI 10.3%-11.1%) compared with patients who did not require intensive care (4.4%, 4.2%-4.5%, P < .001). In multivariable analysis, factors associated with newly diagnosed AF during sepsis included older age, white race, acute organ dysfunction, intensive care unit admission, mechanical ventilation, right heart catheterization, diagnosis of endocarditis, and coronary artery bypass graft surgery. Cardiovascular comorbid conditions generally were not associated with increased risk for newly diagnosed AF during sepsis.
Conclusions: Atrial fibrillation is common among critically ill patients with sepsis. Acute factors, rather than preexisting cardiovascular comorbid conditions, are associated with increased risk for newly diagnosed AF during sepsis, suggesting that mechanisms of newly diagnosed AF during sepsis may differ from the general population of patients with AF.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures
References
-
- Minino AM, Xu J, Kochanek KD, Tejada-Vera B. Death in the United States, 2007. NCHS Data Brief. 2009;(26):1–8. - PubMed
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–1655. - PubMed
-
- Salman S, Bajwa A, Gajic O, et al. Paroxysmal atrial fibrillation in critically ill patients with sepsis. J Intensive Care Med. 2008;23:178–183. - PubMed
-
- Christian SA, Schorr C, Ferchau L, et al. Clinical characteristics and outcomes of septic patients with new-onset atrial fibrillation. J Crit Care. 2008;23:532–536. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
