

Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease
- PMID: 23708168
- PMCID: PMC3664840
- DOI: 10.1016/j.ahj.2013.03.001
Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease
Abstract
Background: Prior trials suggest it is safe to defer transfusion at hemoglobin levels above 7 to 8 g/dL in most patients. Patients with acute coronary syndrome may benefit from higher hemoglobin levels.
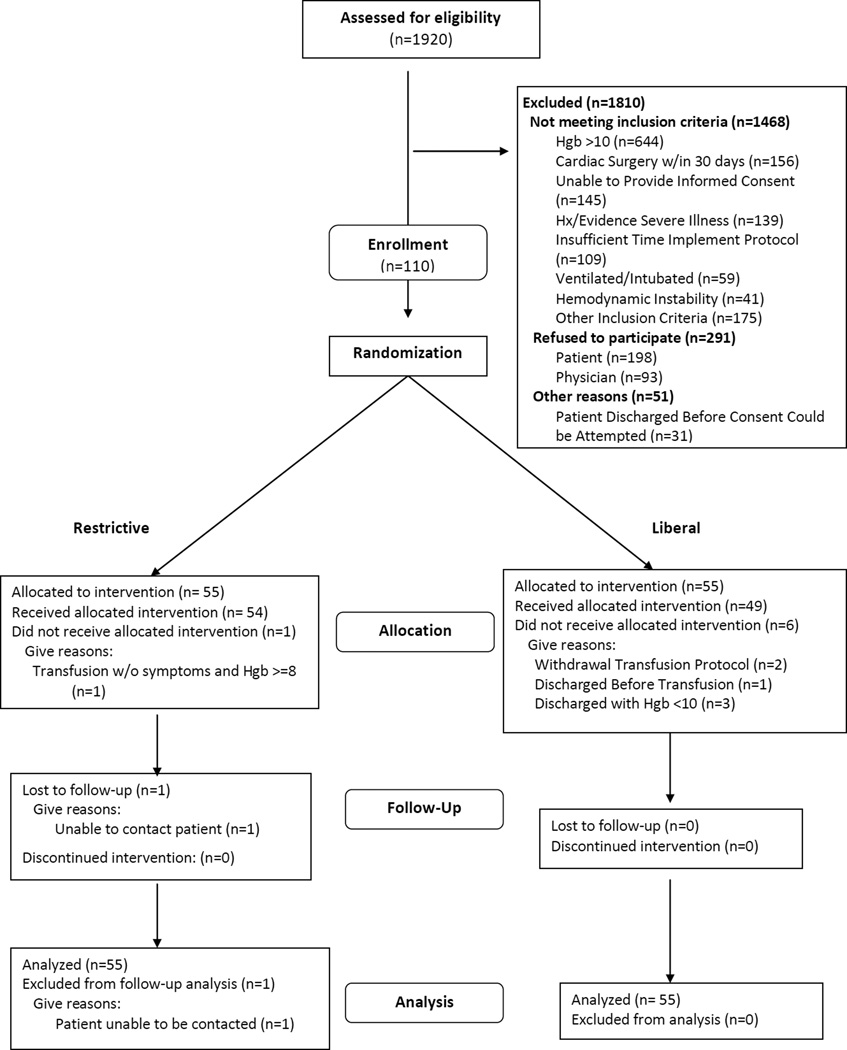
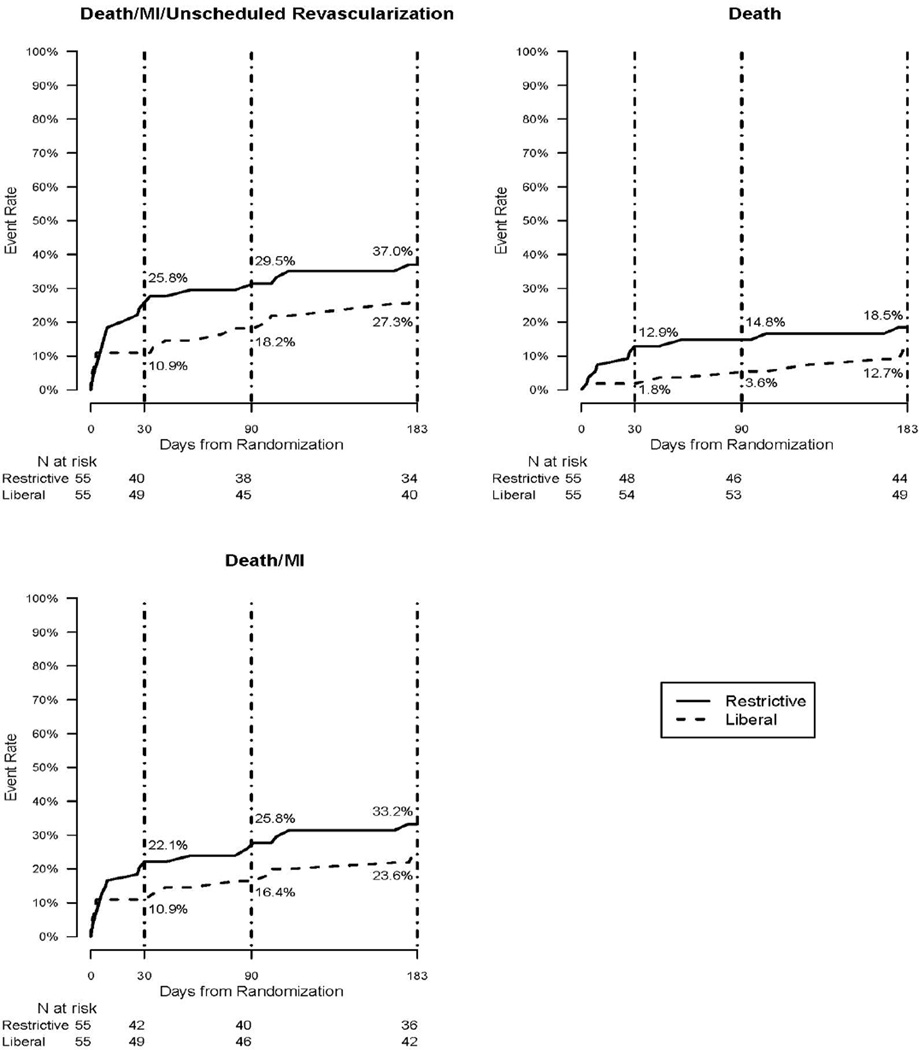
Methods: We performed a pilot trial in 110 patients with acute coronary syndrome or stable angina undergoing cardiac catheterization and a hemoglobin <10 g/dL. Patients in the liberal transfusion strategy received one or more units of blood to raise the hemoglobin level ≥10 g/dL. Patients in the restrictive transfusion strategy were permitted to receive blood for symptoms from anemia or for a hemoglobin <8 g/dL. The predefined primary outcome was the composite of death, myocardial infarction, or unscheduled revascularization 30 days post randomization.
Results: Baseline characteristics were similar between groups except age (liberal, 67.3; restrictive, 74.3). The mean number of units transfused was 1.6 in the liberal group and 0.6 in the restrictive group. The primary outcome occurred in 6 patients (10.9%) in the liberal group and 14 (25.5%) in the restrictive group (risk difference = 15.0%; 95% confidence interval of difference 0.7% to 29.3%; P = .054 and adjusted for age P = .076). Death at 30 days was less frequent in liberal group (n = 1, 1.8%) compared to restrictive group (n = 7, 13.0%; P = .032).
Conclusions: The liberal transfusion strategy was associated with a trend for fewer major cardiac events and deaths than a more restrictive strategy. These results support the feasibility of and the need for a definitive trial.
Trial registration: ClinicalTrials.gov NCT01167582.
Copyright © 2013 Mosby, Inc. All rights reserved.
Comment in
-
Liberal versus restrictive transfusion strategy for patients with coronary artery disease.Am Heart J. 2013 Oct;166(4):e25. doi: 10.1016/j.ahj.2013.07.021. Epub 2013 Aug 15. Am Heart J. 2013. PMID: 24093865 No abstract available.
-
Response to Dr Sandar et al.Am Heart J. 2013 Oct;166(4):e27-8. doi: 10.1016/j.ahj.2013.07.022. Epub 2013 Aug 29. Am Heart J. 2013. PMID: 24093866 No abstract available.
References
-
- Napolitano LM, Kurek S, Luchette FA, Corwin HL, Barie PS, Tisherman SA, et al. Clinical practice guideline: red blood cell transfusion in adult trauma and critical care. Crit Care Med. 2009;37(12):3124–3157. - PubMed
-
- Carson JL, Grossman BJ, Kleinman S, Tinmouth AT, Marques MB, Fung MK, et al. Red Blood Cell Transfusion: A Clinical Practice Guideline From the AABB*. Ann Intern Med. 2012;157(1):49–58. - PubMed
-
- Salisbury AC, Amin AP, Reid KJ, Wang TY, Masoudi FA, Chan PS, et al. Hospital-acquired anemia and in-hospital mortality in patients with acute myocardial infarction. American heart journal. 2011;162(2):300–309. e3. - PubMed
-
- Carson JL, Duff A, Poses RM, Berlin JA, Spence RK, Trout R, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055–1060. - PubMed
-
- Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of Blood Transfusion With Increased Mortality in Myocardial Infarction: A Meta-analysis and Diversity-Adjusted Study Sequential Analysis. JAMA internal medicine. 2013;173(2):132–139. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
