

Advanced respiratory motion compensation for coronary MR angiography
- PMID: 23708271
- PMCID: PMC3715228
- DOI: 10.3390/s130606882
Advanced respiratory motion compensation for coronary MR angiography
Abstract
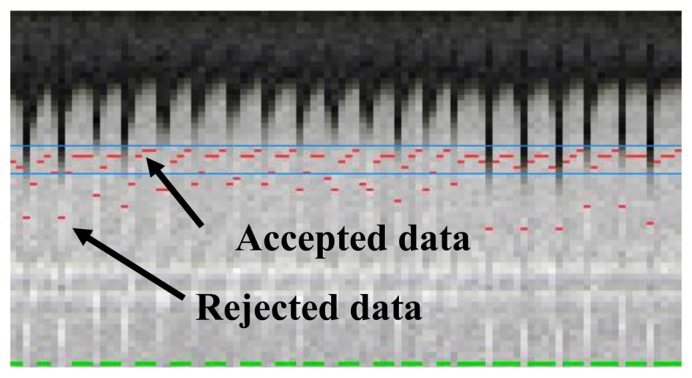
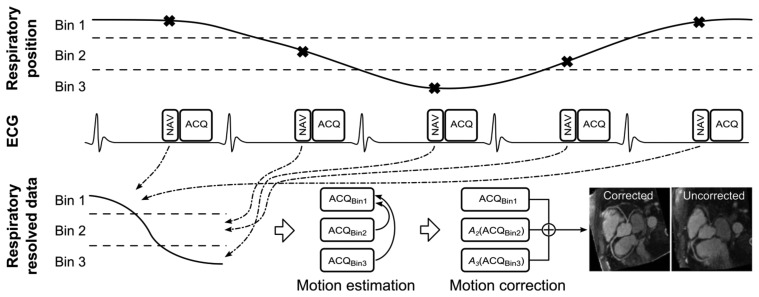
Despite technical advances, respiratory motion remains a major impediment in a substantial amount of patients undergoing coronary magnetic resonance angiography (CMRA). Traditionally, respiratory motion compensation has been performed with a one-dimensional respiratory navigator positioned on the right hemi-diaphragm, using a motion model to estimate and correct for the bulk respiratory motion of the heart. Recent technical advancements has allowed for direct respiratory motion estimation of the heart, with improved motion compensation performance. Some of these new methods, particularly using image-based navigators or respiratory binning, allow for more advanced motion correction which enables CMRA data acquisition throughout most or all of the respiratory cycle, thereby significantly reducing scan time. This review describes the three components typically involved in most motion compensation strategies for CMRA, including respiratory motion estimation, gating and correction, and how these processes can be utilized to perform advanced respiratory motion compensation.
Figures
References
-
- Dewey M. Coronary CT versus MR angiography: Pro CT—The role of CT angiography. Radiology. 2011;258:329–339. - PubMed
-
- Wang Y., Riederer S.J., Ehman R.L. Respiratory motion of the heart-kinematics and the implications for the spatial-resolution in coronary imaging. Magn. Reson. Med. 1995;33:713–719. - PubMed
-
- Keegan J., Gatehouse P., Yang G.Z., Firmin D. Coronary artery motion with the respiratory cycle during breath-holding and free-breathing: Implications for slice-followed coronary artery imaging. Magn. Reson. Med. 2002;47:476–481. - PubMed
-
- Danias P.G., Stuber M., Botnar R.M., Kissinger K.V., Edelman R.R., Manning W.J. Relationship between motion of coronary arteries and diaphragm during free breathing: Lessons from real-time MR imaging. Am. J. Roentgenol. 1999;172:1061–1065. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
