

Risk factors for adverse outcomes by left ventricular ejection fraction in a contemporary heart failure population
- PMID: 23709659
- PMCID: PMC3826979
- DOI: 10.1161/CIRCHEARTFAILURE.112.000180
Risk factors for adverse outcomes by left ventricular ejection fraction in a contemporary heart failure population
Abstract
Background: Although heart failure (HF) is a syndrome with important differences in response to therapy by left ventricular ejection fraction (LVEF), existing risk stratification models typically group all HF patients together. The relative importance of common predictor variables for important clinical outcomes across strata of LVEF is relatively unknown.
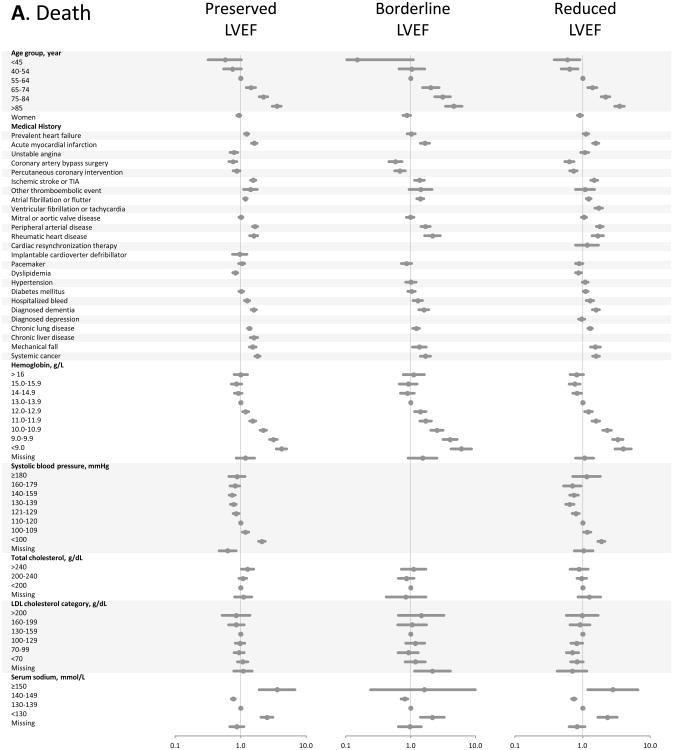
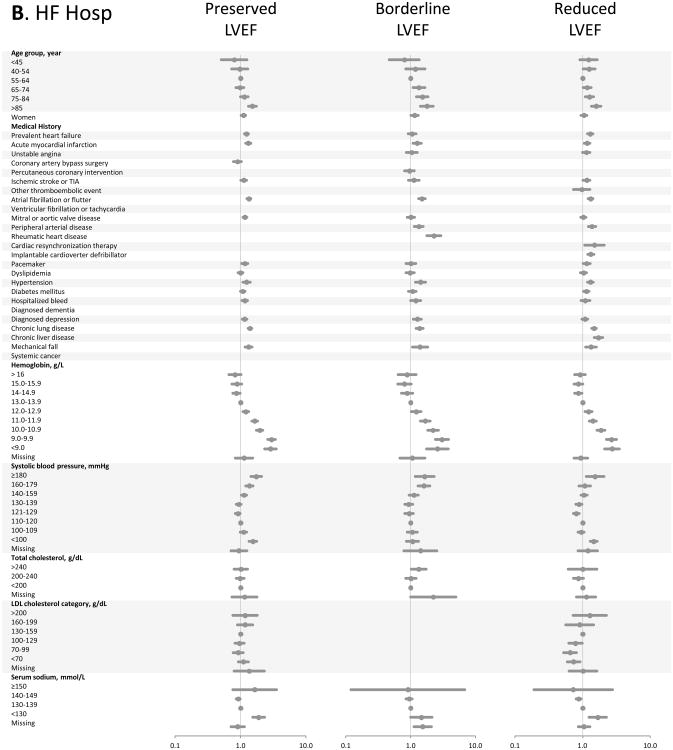
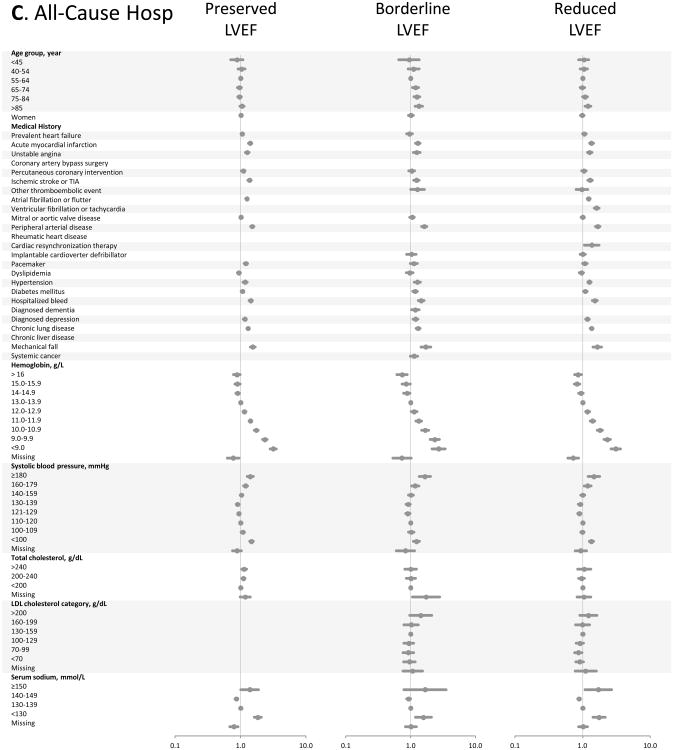
Methods and results: We identified all members with HF between 2005 and 2008 from 4 integrated healthcare systems in the Cardiovascular Research Network. LVEF was categorized as preserved (LVEF ≥ 50% or normal), borderline (41%-49% or mildly reduced), and reduced (≤ 40% or moderately to severely reduced). We used Cox regression models to identify independent predictors of death and hospitalization by LVEF category. Among 30094 ambulatory adults with HF, mean age was 74 years and 46% were women. LVEF was preserved in 49.5%, borderline in 16.2%, and reduced in 34.3% of patients. During a median follow-up of 1.8 years (interquartile range, 0.8-3.1), 8060 (26.8%) patients died, 8108 (26.9%) were hospitalized for HF, and 20272 (67.4%) were hospitalized for any reason. In multivariable models, nearly all tested covariates performed similarly across LVEF strata for the outcome of death from any cause, as well as for HF-related and all-cause hospitalizations.
Conclusions: We found that in a large, diverse contemporary HF population, risk assessment was strikingly similar across all LVEF categories. These data suggest that, although many HF therapies are uniquely applied to patients with reduced LVEF, individual prognostic factor performance does not seem to be significantly related to level of left ventricular systolic function.
Keywords: heart failure; outcomes assessment (health care); prognosis; risk factors.
Conflict of interest statement
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics--2013 Update: A Report From the American Heart Association. Circulation. 2013;127:e6–e245. - PMC - PubMed
-
- Hlatky MA, Greenland P, Arnett DK, Ballantyne CM, Criqui MH, Elkind MS, Go AS, Harrell FE, Jr, Hong Y, Howard BV, Howard VJ, Hsue PY, Kramer CM, McConnell JP, Normand SL, O'Donnell CJ, Smith SC, Jr, Wilson PW. Criteria for evaluation of novel markers of cardiovascular risk: A scientific statement from the american heart association. Circulation. 2009;119:2408–2416. - PMC - PubMed
-
- Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: Derivation and validation of a clinical model. JAMA. 2003;290:2581–2587. - PubMed
-
- Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD, Cropp AB, Anand I, Maggioni A, Burton P, Sullivan MD, Pitt B, Poole-Wilson PA, Mann DL, Packer M. The seattle heart failure model: Prediction of survival in heart failure. Circulation. 2006;113:1424–1433. - PubMed
-
- Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation. 1997;95:2660–2667. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
