

The NOMS framework: approach to the treatment of spinal metastatic tumors
- PMID: 23709750
- PMCID: PMC4063402
- DOI: 10.1634/theoncologist.2012-0293
The NOMS framework: approach to the treatment of spinal metastatic tumors
Abstract
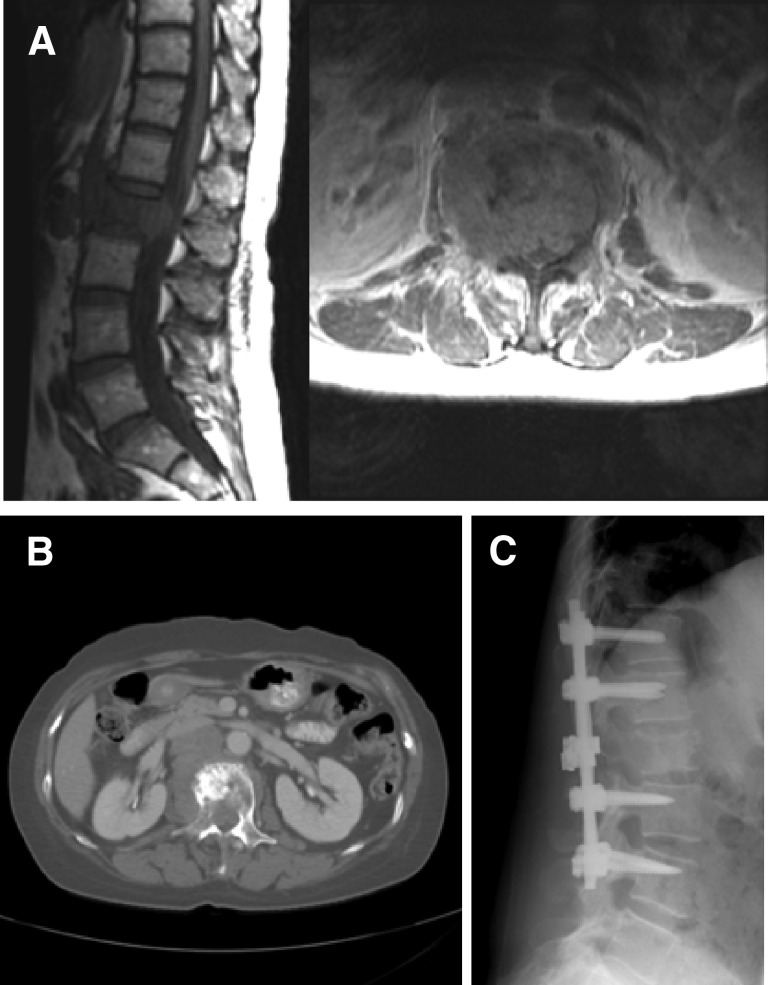
Background: Spinal metastases frequently arise in patients with cancer. Modern oncology provides numerous treatment options that include effective systemic, radiation, and surgical options. We delineate and provide the evidence for the neurologic, oncologic, mechanical, and systemic (NOMS) decision framework, which is used at Memorial Sloan-Kettering Cancer Center to determine the optimal therapy for patients with spine metastases.
Methods: We provide a literature review of the integral publications that serve as the basis for the NOMS framework and report the results of systematic implementation of the NOMS-guided treatment.
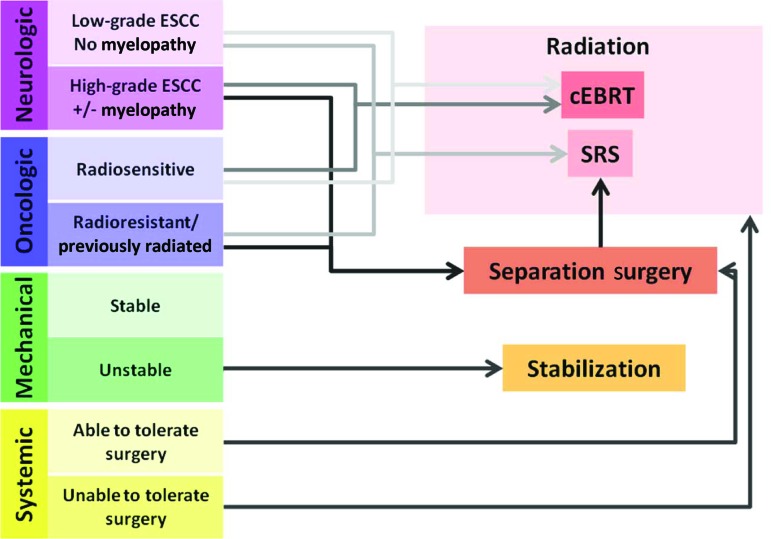
Results: The NOMS decision framework consists of the neurologic, oncologic, mechanical, and systemic considerations and incorporates the use of conventional external beam radiation, spinal stereotactic radiosurgery, and minimally invasive and open surgical interventions. Review of radiation oncology and surgical literature that examine the outcomes of treatment of spinal metastatic tumors provides support for the NOMS decision framework. Application of the NOMS paradigm integrates multimodality therapy to optimize local tumor control, pain relief, and restoration or preservation of neurologic function and minimizes morbidity in this often systemically ill patient population.
Conclusion: NOMS paradigm provides a decision framework that incorporates sentinel decision points in the treatment of spinal metastases. Consideration of the tumor sensitivity to radiation in conjunction with the extent of epidural extension allows determination of the optimal radiation treatment and the need for surgical decompression. Mechanical stability of the spine and the systemic disease considerations further help determine the need and the feasibility of surgical intervention.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Cobb CA, 3rd, Leavens ME, Eckles N. Indications for nonoperative treatment of spinal cord compression due to breast cancer. J Neurosurg. 1977;47:653–658. - PubMed
-
- Walsh GL, Gokaslan ZL, McCutcheon IE, et al. Anterior approaches to the thoracic spine in patients with cancer: Indications and results. Ann Thorac Surg. 1997;64:1611–1618. - PubMed
-
- Barron KD. Experiences with metastatic neoplasms involving the spinal cord. Neurology. 1959;9:91–106. - PubMed
-
- Bach F. Metastatic spinal cord compression. Occurrence, symptoms, clinical presentations and prognosis in 398 patients with spinal cord compression. Acta neurochirurgica. 1990;107:37–43. - PubMed
-
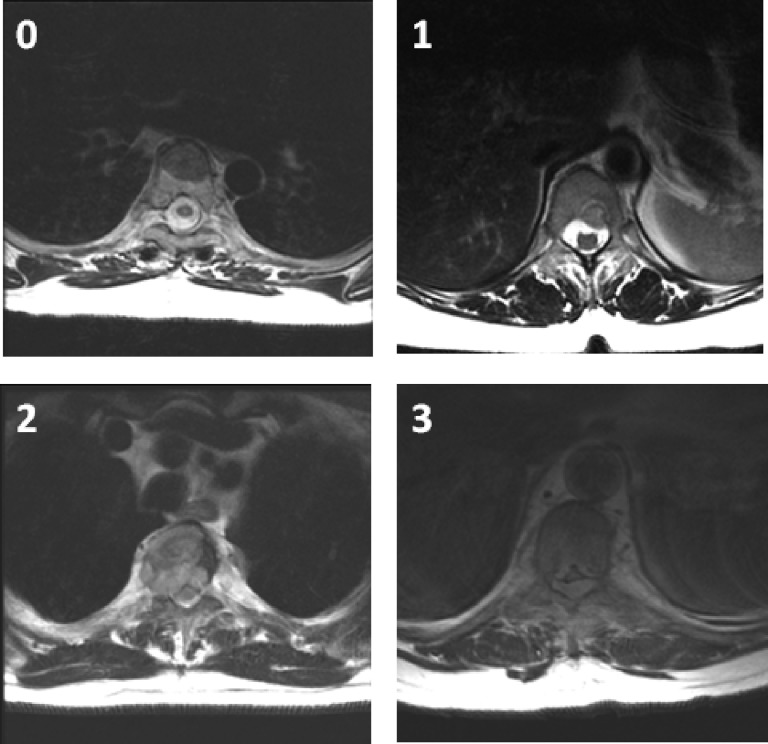
- Bilsky MH, Laufer I, Fourney DR, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. 2010;13:324–328. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
