

Splenic anomalies of shape, size, and location: pictorial essay
- PMID: 23710135
- PMCID: PMC3654276
- DOI: 10.1155/2013/321810
Splenic anomalies of shape, size, and location: pictorial essay
Abstract
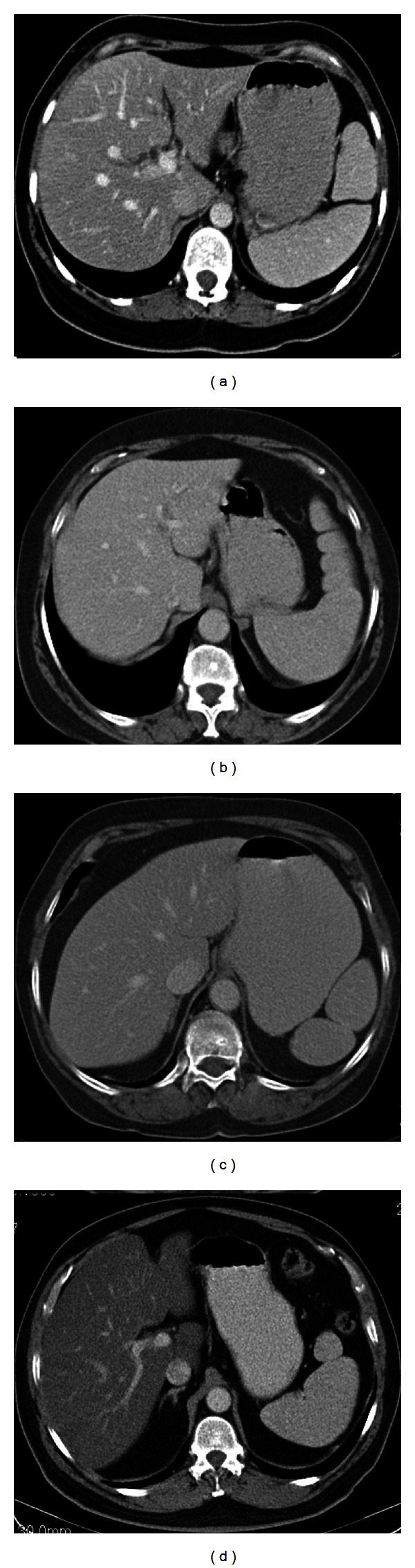
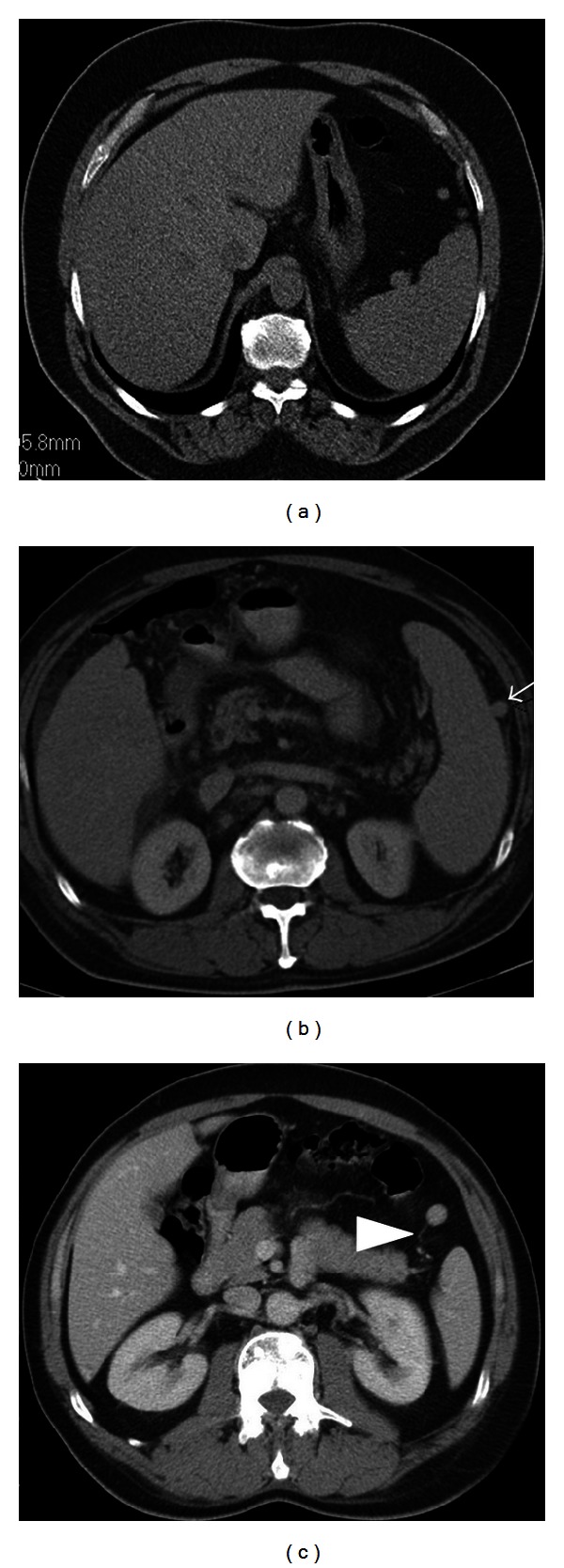
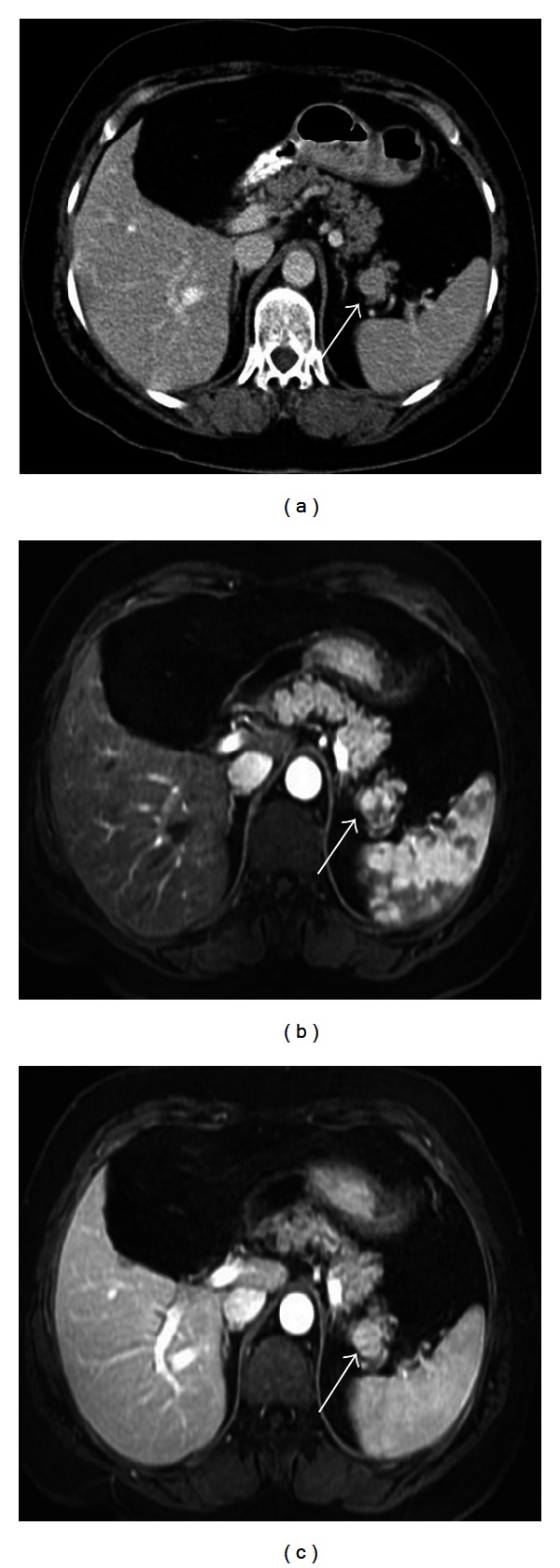
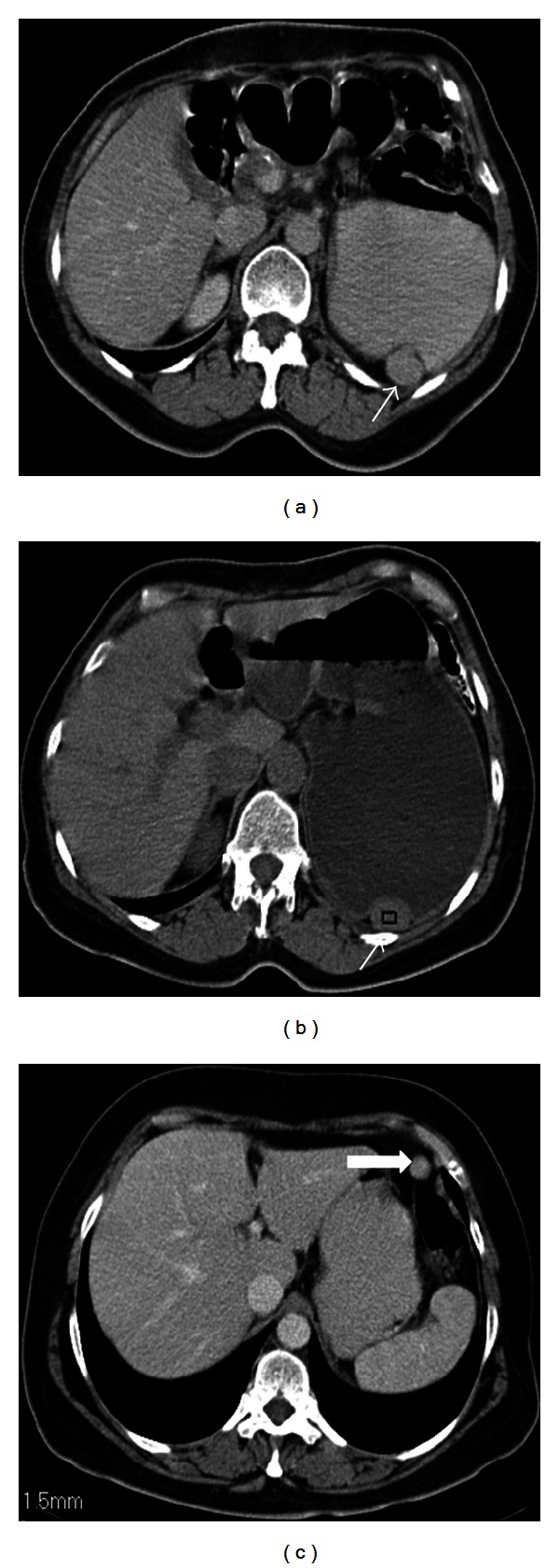
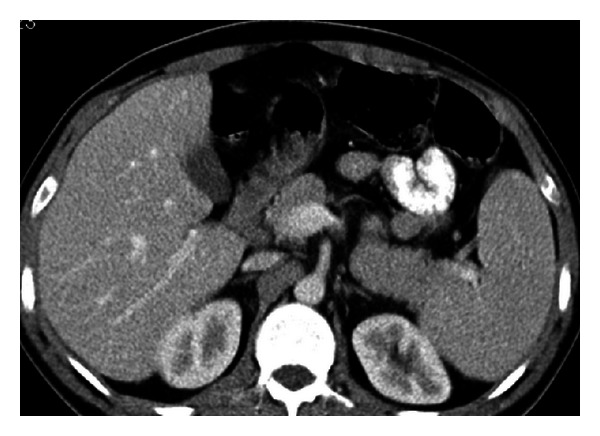
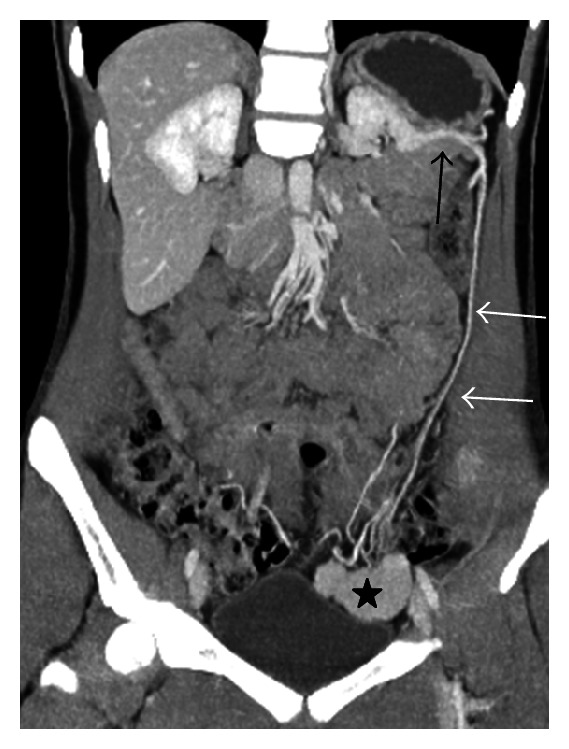
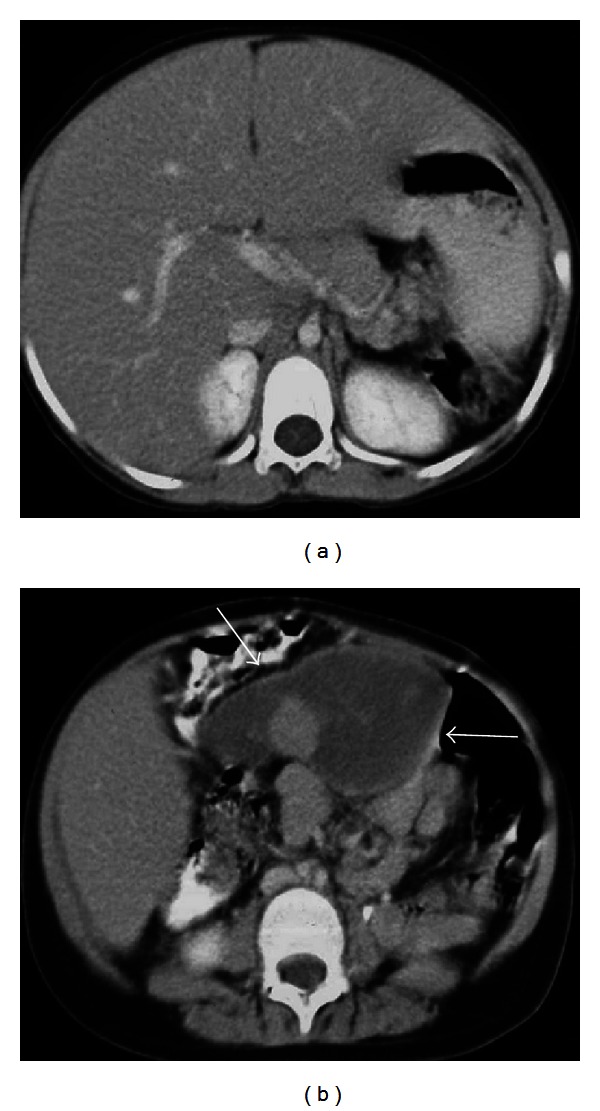
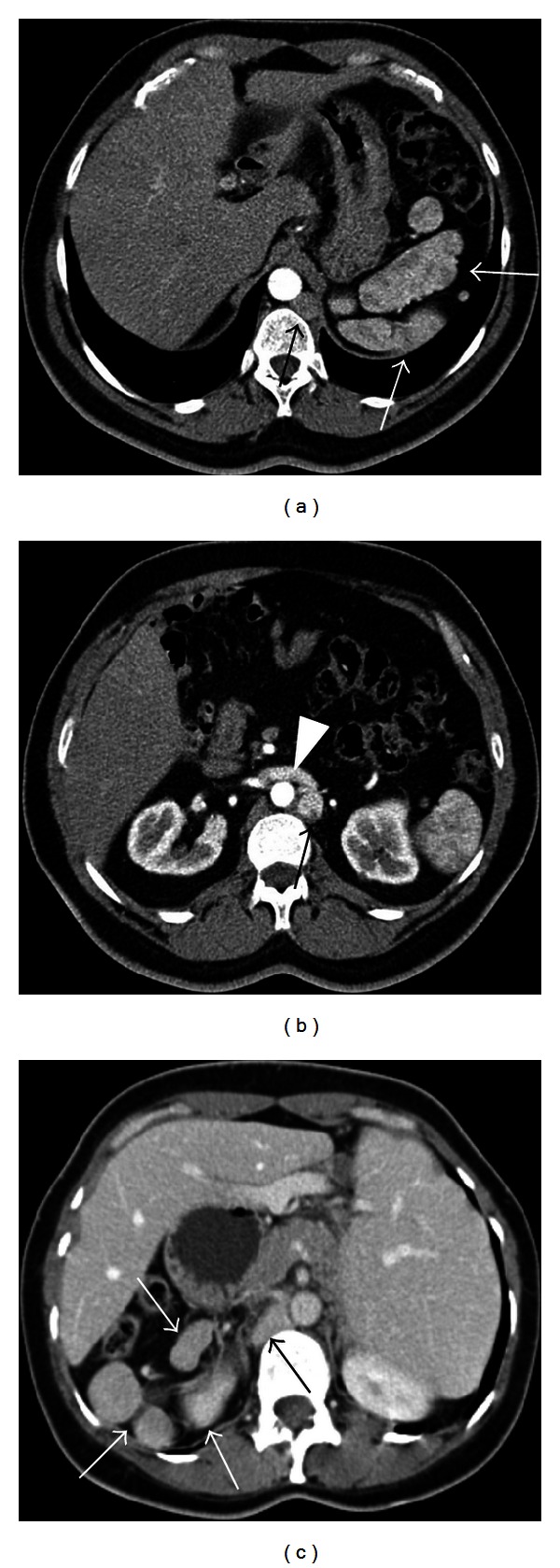
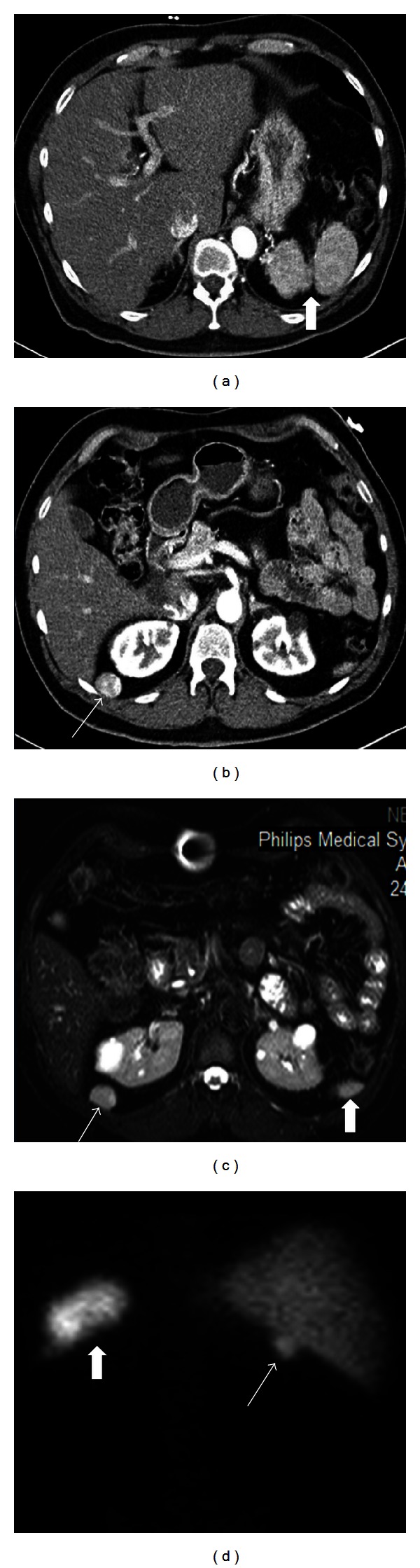
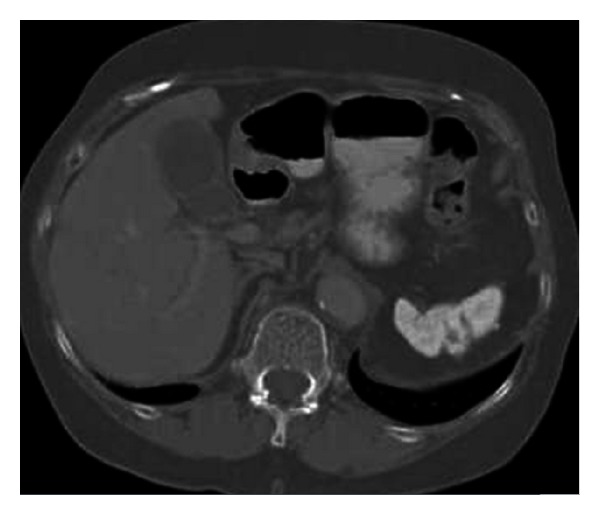
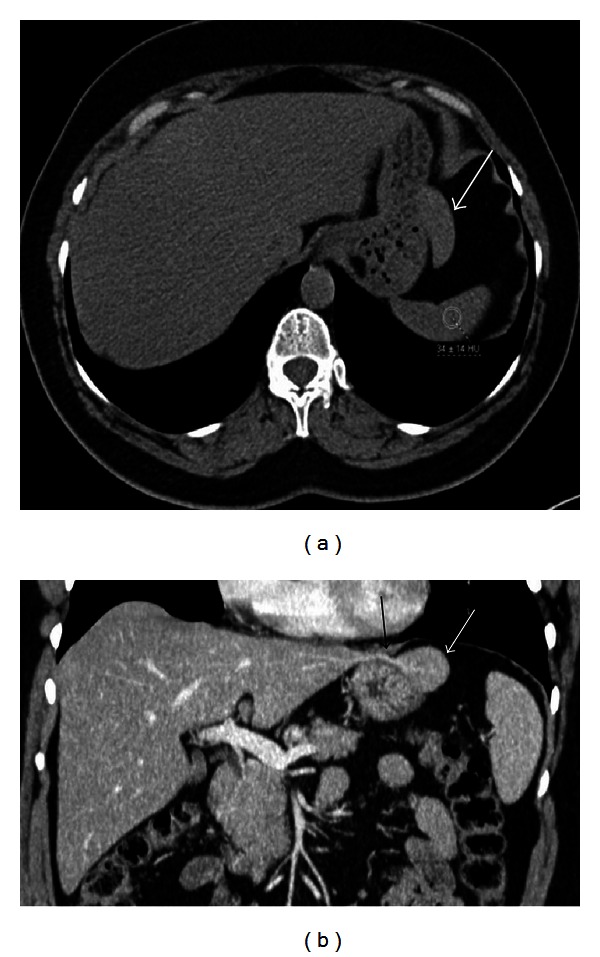
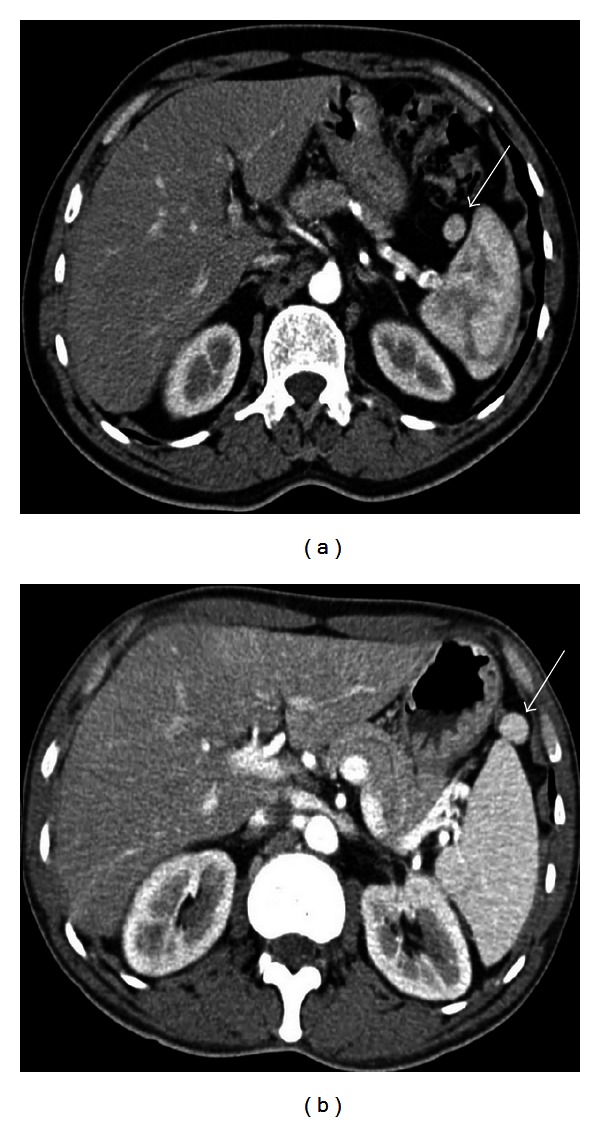
Spleen can have a wide range of anomalies including its shape, location, number, and size. Although most of these anomalies are congenital, there are also acquired types. Congenital anomalies affecting the shape of spleen are lobulations, notches, and clefts; the fusion and location anomalies of spleen are accessory spleen, splenopancreatic fusion, and wandering spleen; polysplenia can be associated with a syndrome. Splenosis and small spleen are acquired anomalies which are caused by trauma and sickle cell disease, respectively. These anomalies can be detected easily by using different imaging modalities including ultrasonography, computed tomography, magnetic resonance imaging, and also Tc-99m scintigraphy. In this pictorial essay, we review the imaging findings of these anomalies which can cause diagnostic pitfalls and be interpreted as pathologic processes.
Figures


References
-
- Gayer G, Zissin R, Apter S, Atar E, Portnoy O, Itzchak Y. CT findings in congenital anomalies of the spleen. British Journal of Radiology. 2001;74(884):767–772. - PubMed
-
- Dodds WJ, Taylor AJ, Erickson SJ, Stewart ET, Lawson TL. Radiologic imaging of splenic anomalies. American Journal of Roentgenology. 1990;155(4):805–810. - PubMed
-
- Rabushka LS, Kawashima A, Fishman EK. Imaging of the spleen: CT with supplemental MR examination. Radiographics. 1994;14(2):307–332. - PubMed
-
- Elsayes KM, Narra VR, Mukundan G, Lewis JS, Menias CO, Heiken JP. MR imaging of the spleen: spectrum of abnormalities. Radiographics. 2005;25(4):967–982. - PubMed
-
- Mortelé KJ, Mortelé B, Silverman SG. CT features of the accessory spleen. American Journalism Review. 2004;183:1653–1657. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
