

The Relation between Obesity and Survival after Surgical Resection of Hepatitis C Virus-Related Hepatocellular Carcinoma
- PMID: 23710167
- PMCID: PMC3655578
- DOI: 10.1155/2013/430438
The Relation between Obesity and Survival after Surgical Resection of Hepatitis C Virus-Related Hepatocellular Carcinoma
Abstract
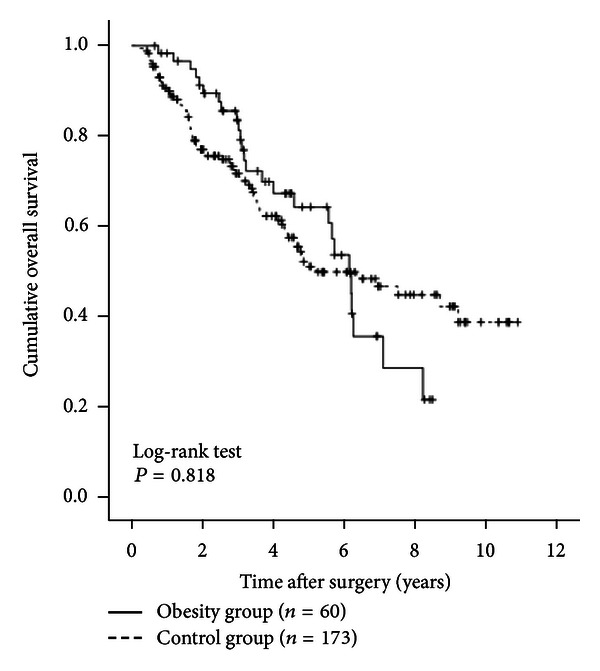
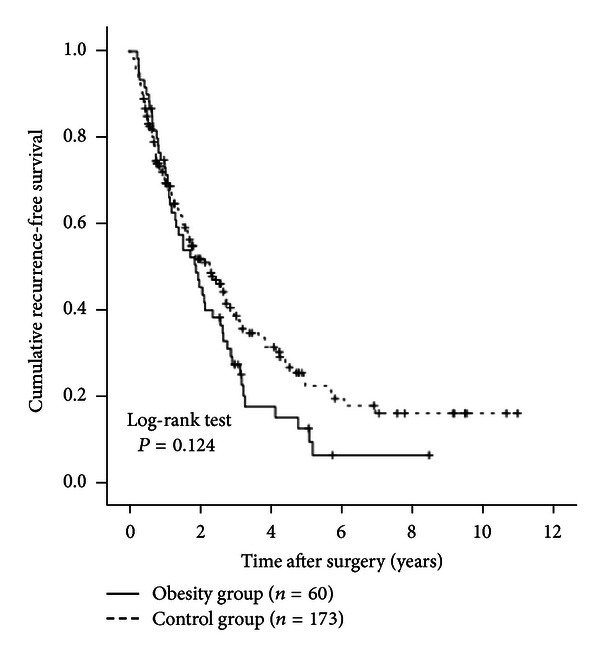
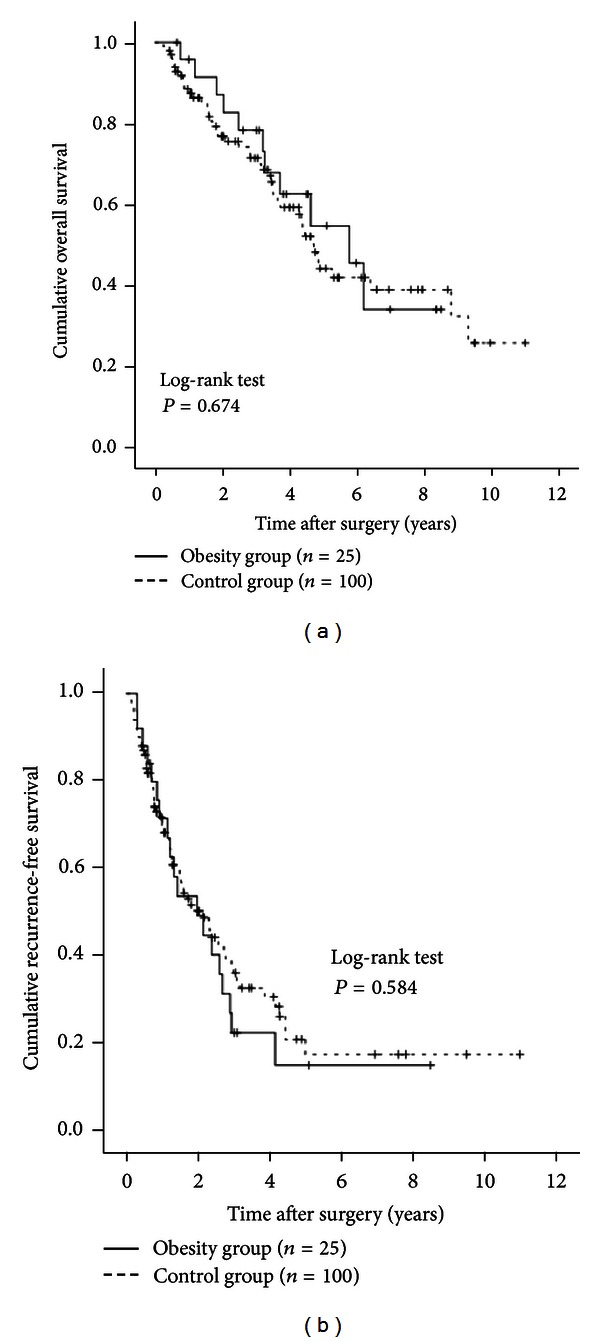
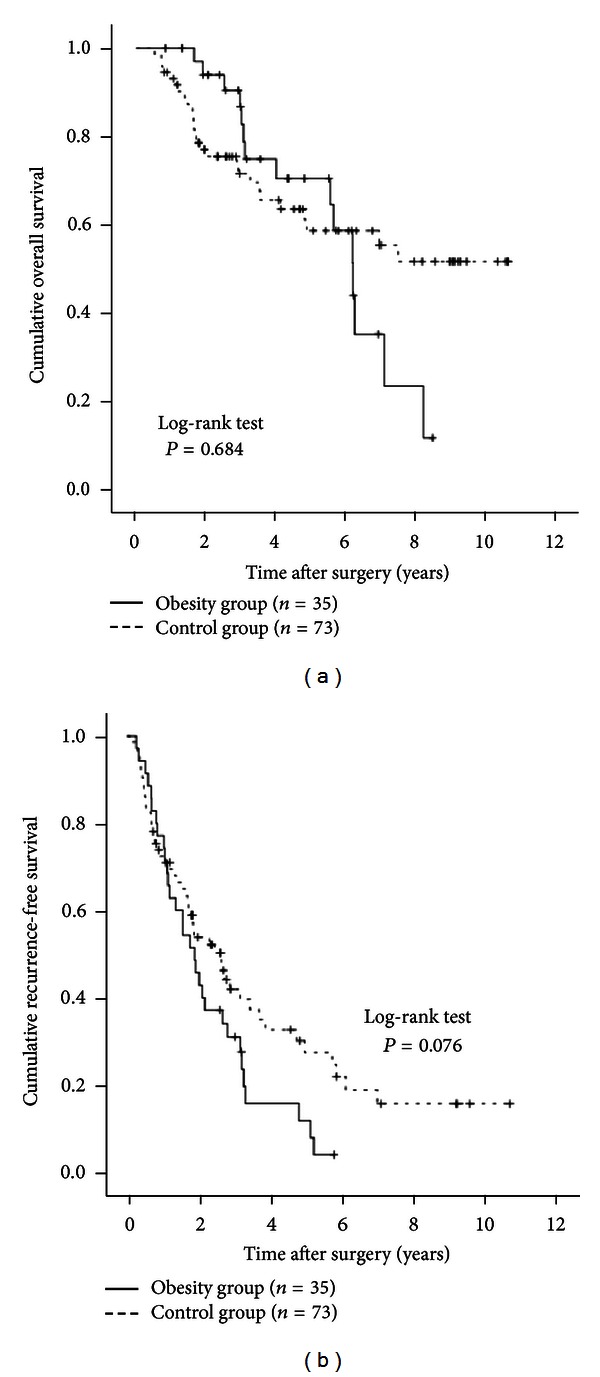
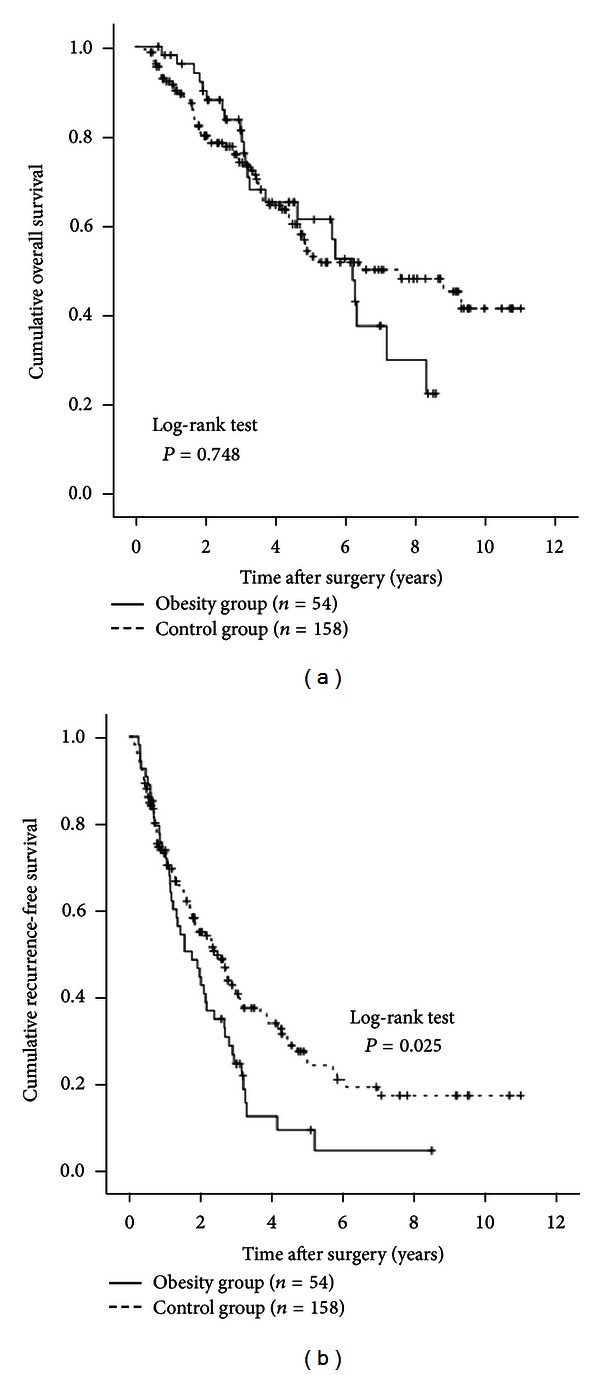
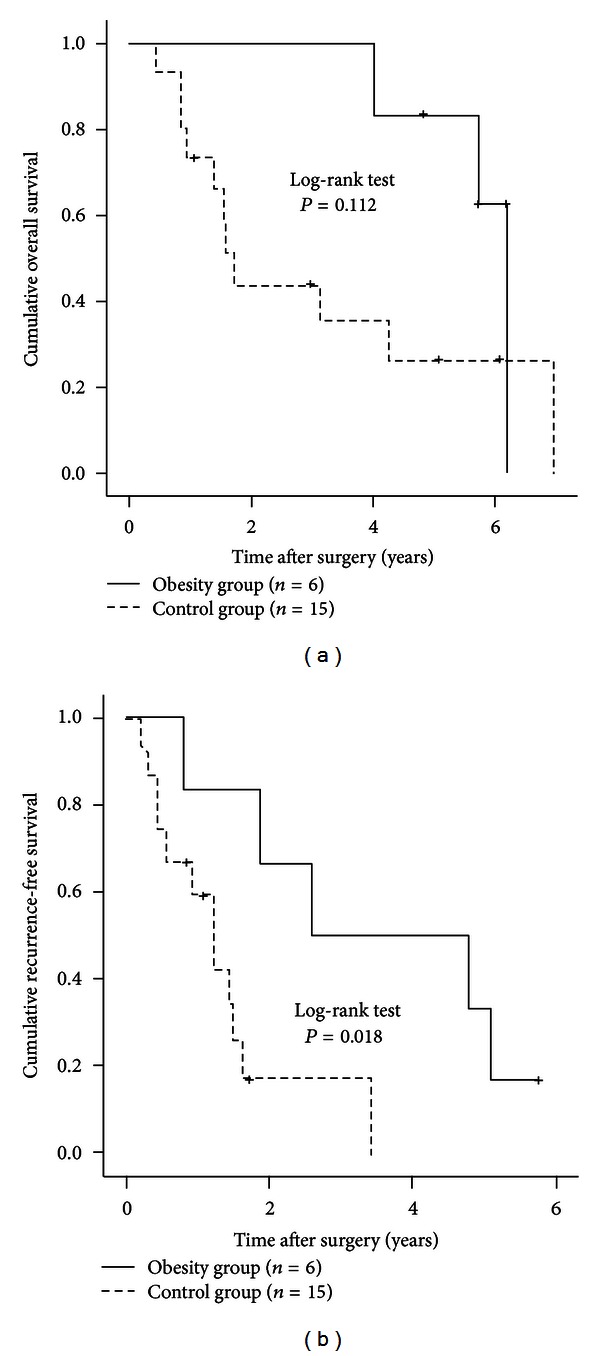
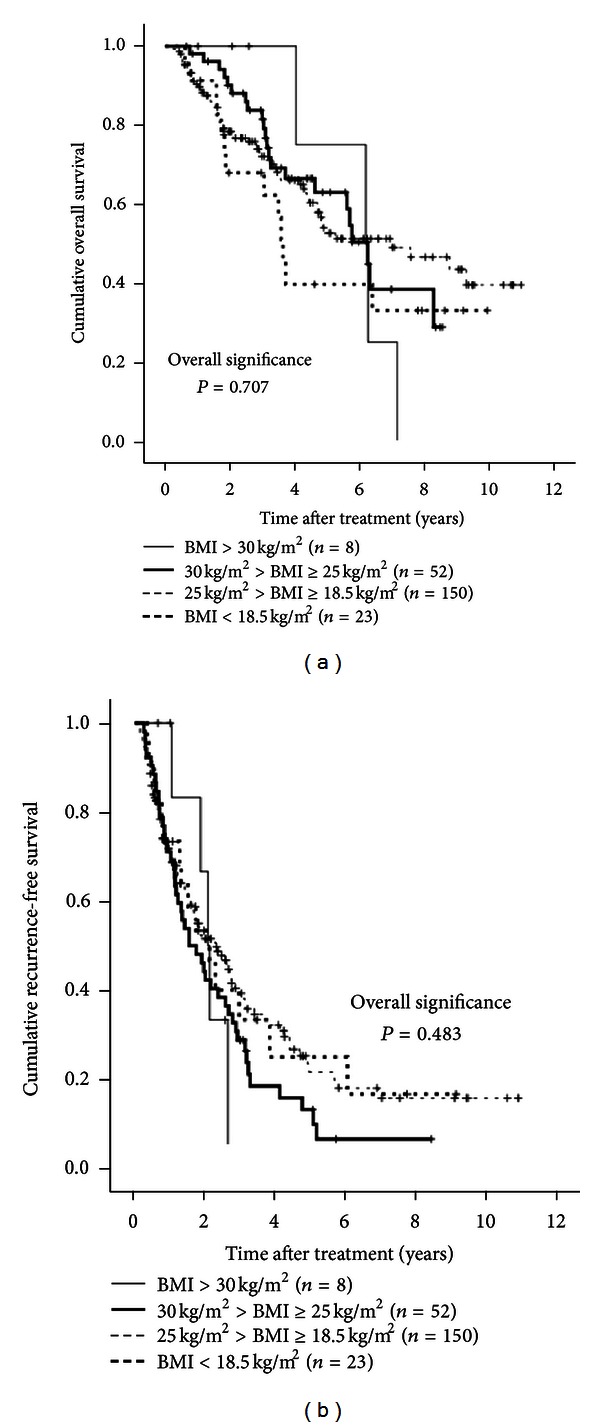
Background and Aims. We aimed to investigate the relationship between obesity and survival in hepatitis C virus-(HCV-) related hepatocellular carcinoma (HCC) patients who underwent curative surgical resection (SR). Methods. A total of 233 patients with HCV-related HCC who underwent curative SR were included. They included 60 patients (25.8%) with a body mass index (BMI) of > 25 kg/m(2) (obesity group) and 173 patients with a BMI of < 25 kg/m(2) (control group). Overall survival (OS) and recurrence-free survival (RFS) rates were compared. Results. The median follow-up periods were 3.6 years in the obesity group and 3.1 years in the control group. The 1-, 3-, and 5-year cumulative OS rates were 98.3%, 81.0%, and 63.9% in the obesity group and 90.0%, 70.5%, and 50.3% in the control group (P = 0.818). The corresponding RFS rates were 70.1%, 27.0%, and 12.0% in the obesity group and 70.1%, 39.0%, and 21.7% in the control group (P = 0.124). There were no significant differences between the obesity group and the control group in terms of blood loss during surgery (P = 0.899) and surgery-related serious adverse events (P = 0.813). Conclusions. Obesity itself did not affect survival in patients with HCV-related HCC after curative SR.
Figures

References
-
- Livraghi T, Mäkisalo H, Line PD. Treatment options in hepatocellular carcinoma today. Scandinavian Journal of Surgery. 2011;100(1):22–29. - PubMed
-
- de Lope CR, Tremosini S, Forner A, Reig M, Bruix J. Management of HCC. Journal of Hepatology. 2012;56(supplement 1):S75–S87. - PubMed
-
- El-Serag HB. Hepatocellular carcinoma. The New England Journal of Medicine. 2011;365:118–1127. - PubMed
-
- Umemura T, Ichijo T, Yoshizawa K, Tanaka E, Kiyosawa K. Epidemiology of hepatocellular carcinoma in Japan. Journal of Gastroenterology. 2009;44(19, supplement):102–107. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
