

Current status of core and advanced adult gastrointestinal endoscopy training in Canada: Survey of existing accredited programs
- PMID: 23712301
- PMCID: PMC3735729
- DOI: 10.1155/2013/186284
Current status of core and advanced adult gastrointestinal endoscopy training in Canada: Survey of existing accredited programs
Abstract
Objective: To determine the current status of core and advanced adult gastroenterology training in Canada.
Methods: A survey consisting of 20 questions pertaining to core and advanced endoscopy training was circulated to 14 accredited adult gastroenterology residency program directors. For continuous variables, median and range were analyzed; for categorical variables, percentage and associated 95% CIs were analyzed.
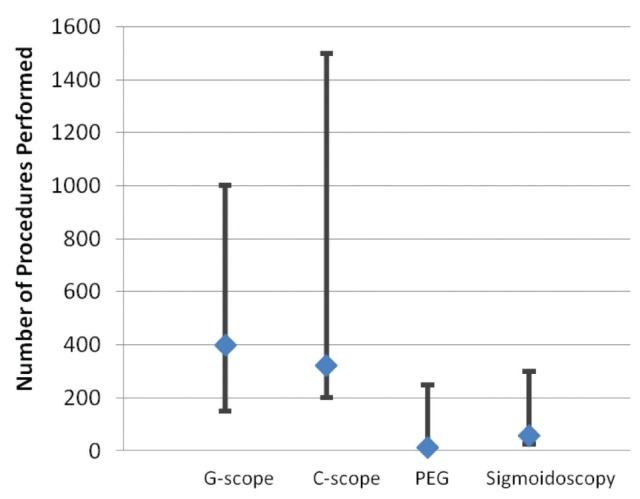
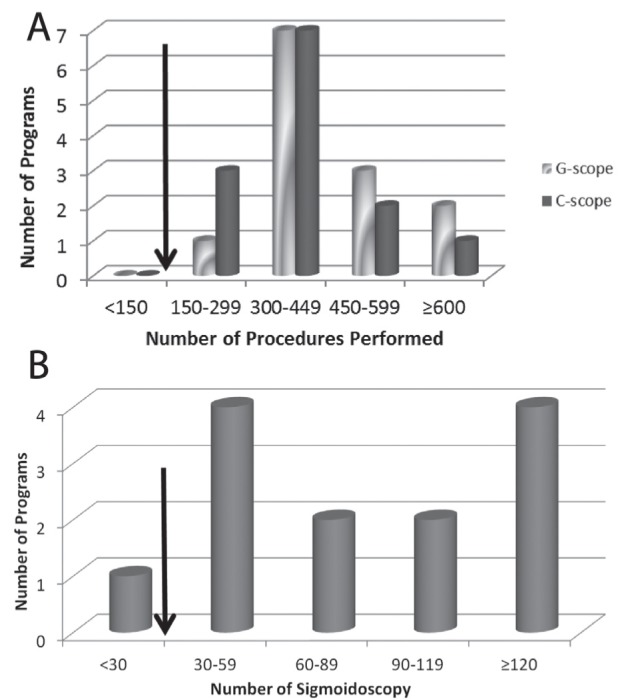
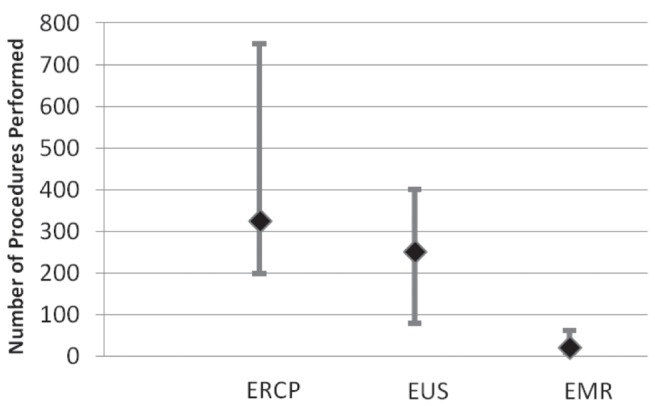
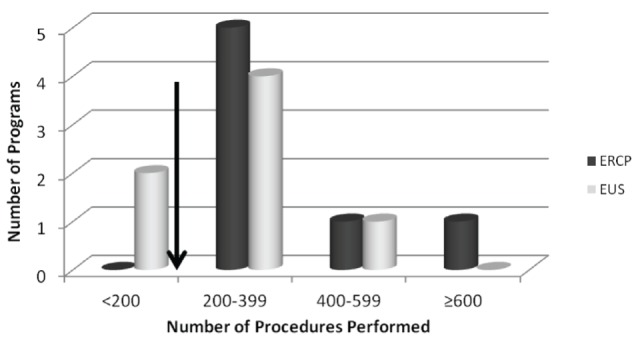
Results: All 14 programs responded to the survey. The median number of core trainees was six (range four to 16). The median (range) procedural volumes for gastroscopy, colonoscopy, percutaneous endoscopic gastrostomy and sigmoidoscopy, respectively, were 400 (150 to 1000), 325 (200 to 1500), 15 (zero to 250) and 60 (25 to 300). Eleven of 13 (84.6%) programs used endoscopy simulators in their curriculum. Eight of 14 programs (57%) provided a structured advanced endoscopy training fellowship. The majority (88%) offered training of combined endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasonography. The median number of positions offered yearly for advanced endoscopy fellowship was one (range one to three). The median (range) procedural volumes for ERCP, endoscopic ultrasonography and endoscopic mucosal resection, respectively, were 325 (200 to 750), 250 (80 to 400) and 20 (10 to 63). None of the current programs offered training in endoscopic submucosal dissection or natural orifice transluminal endoscopic surgery.
Conclusion: Most accredited adult Canadian gastroenterology programs met the minimal procedural requirements recommended by the Canadian Association of Gastroenterology during core training. However, a more heterogeneous experience has been observed for advanced training. Additional studies would be required to validate and standardize evaluation tools used during gastroenterology curricula.
OBJECTIF :: Déterminer l’état actuel de la formation en gastroentérologie au Canada.
MÉTHODE :: Un sondage de 20 questions sur la formation de base et avancée a été distribué aux directeurs des programmes de gastroentérologie accrédités au Canada. La médiane et l’étendue des variables continues, ainsi que le pourcentage et les intervalles de confiance à 95% des variables catégorielles, ont été analysés.
RÉSULTATS :: Les 14 programmes ont répondu au sondage. La médiane du nombre des résidents en formation de base était de 6 (l’étendue étant de 4 à 16). Le nombre de gastroscopies, coloscopies, gastrostomies percutanées endoscopiques et sigmoïdoscopies était respectivement: 400 (150–1000), 325 (200–1500), 15 (0–250) et 60 (25–300). Onze programmes (84,6%) ont intégrés l’utilisation de simulateurs d’endoscopie dans leur formation. Huit programmes (57%) offraient une formation avancée en endoscopie. La majorité (88%) incluait la combinaison de cholangio-pancréatographie rétrograde endoscopique (CPRE) et d’endosonographie (EUS) durant la formation. La médiane du nombre de postes offerts par année était de 1 (–3). Le nombre de CPRE, EUS et mucosectomies endoscopiques était respectivement: 325 (200–750), 250 (80–400) et 20 (10–63). Aucun programme n’offrait de formation sur la dissection sous-muqueuse endoscopique ou la chirurgie endoscopique transluminale par orifice naturel.
CONCLUSION :: En ce qui concerne la formation de base, la majorité des programmes canadiens satisfaisaient les normes recommandées par l’Association Canadienne de Gastroentérologie. Toutefois, on a observé une plus grande variabilité pour les programmes de formation avancée. De futures études seront nécessaires afin de valider les instruments d’évaluation utilisés dans la formation en endoscopie.
Figures
References
-
- Azad J, Verma D, Kapadia A, Adler D. Can U.S. GI fellowship programs meet American Society for Gastrointestinal Endoscopy recommendations for training in EUS? A survey of U.S. GI fellowship program directors. Gastrointest Endosc. 2006;64:235–41. - PubMed
-
- Trindade AJ, Faulx A, DiMaio CJ. Perspectives on the advanced endoscopy fellowship match. Gastrointest Endosc. 2012;75:650–2. - PubMed
-
- Hawes RH. Advanced endoscopy and endosurgical procedures: Do we need a new subspecialty? Gastrointest Endosc Clin N Am. 2007;17:635–9. ix. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous