

In antibody-positive first-degree relatives of patients with type 1 diabetes, HLA-A*24 and HLA-B*18, but not HLA-B*39, are predictors of impending diabetes with distinct HLA-DQ interactions
- PMID: 23712485
- PMCID: PMC3918938
- DOI: 10.1007/s00125-013-2951-8
In antibody-positive first-degree relatives of patients with type 1 diabetes, HLA-A*24 and HLA-B*18, but not HLA-B*39, are predictors of impending diabetes with distinct HLA-DQ interactions
Abstract
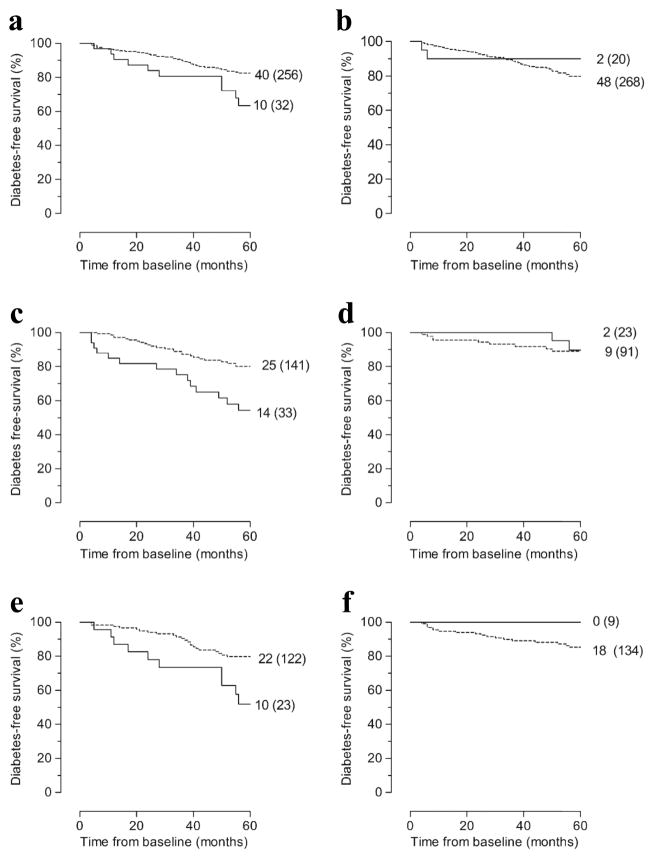
Aims/hypothesis: Secondary type 1 diabetes prevention trials require selection of participants with impending diabetes. HLA-A and -B alleles have been reported to promote disease progression. We investigated whether typing for HLA-B*18 and -B*39 may complement screening for HLA-DQ8, -DQ2 and -A*24 and autoantibodies (Abs) against islet antigen-2 (IA-2) and zinc transporter 8 (ZnT8) for predicting rapid progression to hyperglycaemia.
Methods: A registry-based group of 288 persistently autoantibody-positive (Ab(+)) offspring/siblings (aged 0-39 years) of known patients (Ab(+) against insulin, GAD, IA-2 and/or ZnT8) were typed for HLA-DQ, -A and -B and monitored from the first Ab(+) sample for development of diabetes within 5 years.
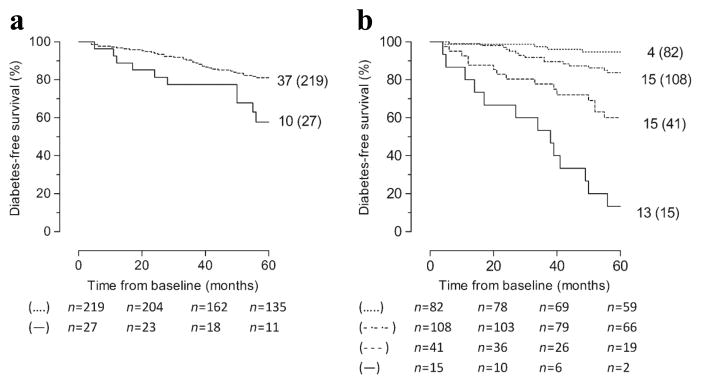
Results: Unlike HLA-B*39, HLA-B*18 was associated with accelerated disease progression, but only in HLA-DQ2 carriers (p < 0.006). In contrast, HLA-A*24 promoted progression preferentially in the presence of HLA-DQ8 (p < 0.002). In HLA-DQ2- and/or HLA-DQ8-positive relatives (n = 246), HLA-B*18 predicted impending diabetes (p = 0.015) in addition to HLA-A*24, HLA-DQ2/DQ8 and positivity for IA-2A or ZnT8A (p ≤ 0.004). HLA-B*18 interacted significantly with HLA-DQ2/DQ8 and HLA-A*24 in the presence of IA-2 and/or ZnT8 autoantibodies (p ≤ 0.009). Additional testing for HLA-B*18 and -A*24 significantly improved screening sensitivity for rapid progressors, from 38% to 53%, among relatives at high Ab-inferred risk carrying at least one genetic risk factor. Screening for HLA-B*18 increased sensitivity for progressors, from 17% to 28%, among individuals carrying ≥ 3 risk markers conferring >85% 5 year risk.
Conclusions/interpretation: These results reinforce the importance of HLA class I alleles in disease progression and quantify their added value for preparing prevention trials.
Conflict of interest statement
DUALITY OF INTEREST
The authors declare that there is no duality of interest associated with this manuscript.
Figures
References
-
- Tait BD, Colman PG, Morahan G, et al. HLA genes associated with autoimmunity and progression to disease in type 1 diabetes. Tissue Antigens. 2003;61:146–153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
