

Economic support to improve tuberculosis treatment outcomes in South Africa: a pragmatic cluster-randomized controlled trial
- PMID: 23714270
- PMCID: PMC3680200
- DOI: 10.1186/1745-6215-14-154
Economic support to improve tuberculosis treatment outcomes in South Africa: a pragmatic cluster-randomized controlled trial
Abstract
Background: Poverty undermines adherence to tuberculosis treatment. Economic support may both encourage and enable patients to complete treatment. In South Africa, which carries a high burden of tuberculosis, such support may improve the currently poor outcomes of patients on tuberculosis treatment. The aim of this study was to test the feasibility and effectiveness of delivering economic support to patients with pulmonary tuberculosis in a high-burden province of South Africa.
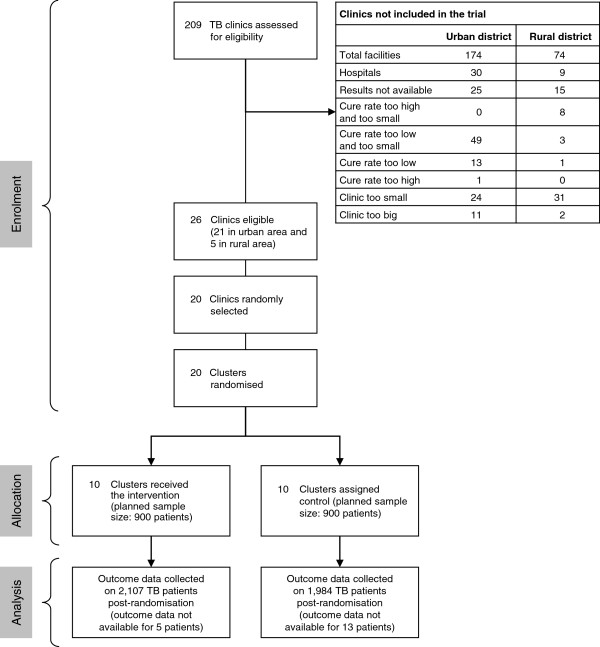
Methods: This was a pragmatic, unblinded, two-arm cluster-randomized controlled trial, where 20 public sector clinics acted as clusters. Patients with pulmonary tuberculosis in intervention clinics (n = 2,107) were offered a monthly voucher of ZAR120.00 (approximately US$15) until the completion of their treatment. Vouchers were redeemed at local shops for foodstuffs. Patients in control clinics (n = 1,984) received usual tuberculosis care.
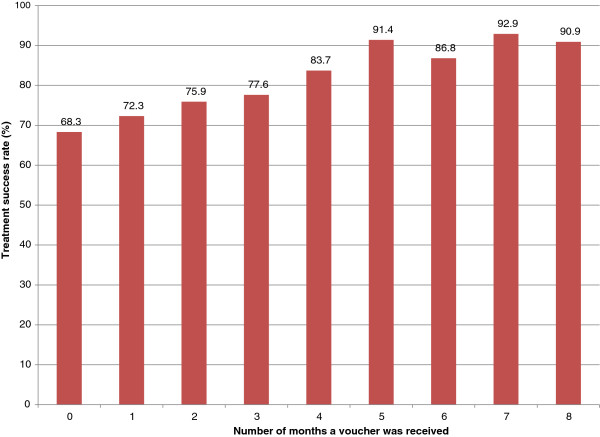
Results: Intention to treat analysis showed a small but non-significant improvement in treatment success rates in intervention clinics (intervention 76.2%; control 70.7%; risk difference 5.6% (95% confidence interval: -1.2%, 12.3%), P = 0.107). Low fidelity to the intervention meant that 36.2% of eligible patients did not receive a voucher at all, 32.3% received a voucher for between one and three months and 31.5% received a voucher for four to eight months of treatment. There was a strong dose-response relationship between frequency of receipt of the voucher and treatment success (P <0.001).
Conclusions: Our pragmatic trial has shown that, in the real world setting of public sector clinics in South Africa, economic support to patients with tuberculosis does not significantly improve outcomes on treatment. However, the low fidelity to the delivery of our voucher meant that a third of eligible patients did not receive it. Among patients in intervention clinics who received the voucher at least once, treatment success rates were significantly improved. Further operational research is needed to explore how best to ensure the consistent and appropriate delivery of such support to those eligible to receive it.
Figures
References
-
- Farmer P. Infections and Inequalities: The modern Plagues. Berkeley and Los Angeles, CA: University of California Press; 2001. The consumption of the poor.
-
- Dubos R, Dubos J. The White Plague: Tuberculosis, Man and Society. New Brunswick, NJ: Rutgers University Press; 1996. xv.
-
- Bates I, Fenton C, Gruber J, Lalloo D, Lara AM, Squire SB, Theobald S, Thomson R, Tolhurst R. Vulnerability to malaria, tuberculosis, and HIV/AIDS infection and disease. Part 1: determinants operating at individual and household level. Lancet Infect Dis. 2004;4(5):267–277. doi: 10.1016/S1473-3099(04)01002-3. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
