

Review
doi: 10.1016/j.hoc.2013.03.001.
Immune thrombocytopenia
Affiliations
- PMID: 23714309
- PMCID: PMC3672858
- DOI: 10.1016/j.hoc.2013.03.001
Item in Clipboard
Review
Immune thrombocytopenia
Hematol Oncol Clin North Am.
2013 Jun.
Abstract
Immune thrombocytopenia (ITP) is a common hematologic disorder characterized by isolated thrombocytopenia. ITP presents as a primary or a secondary form. ITP may affect individuals of all ages, with peaks during childhood and in the elderly, in whom the age-specific incidence of ITP is greatest. Bleeding is the most common clinical manifestation of ITP. The pathogenesis of ITP is complex, involving alterations in humoral and cellular immunity. Corticosteroids remain the most common first line therapy for ITP. This article summarizes the classification and diagnosis of primary and secondary ITP, as well as the pathogenesis and options for treatment.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
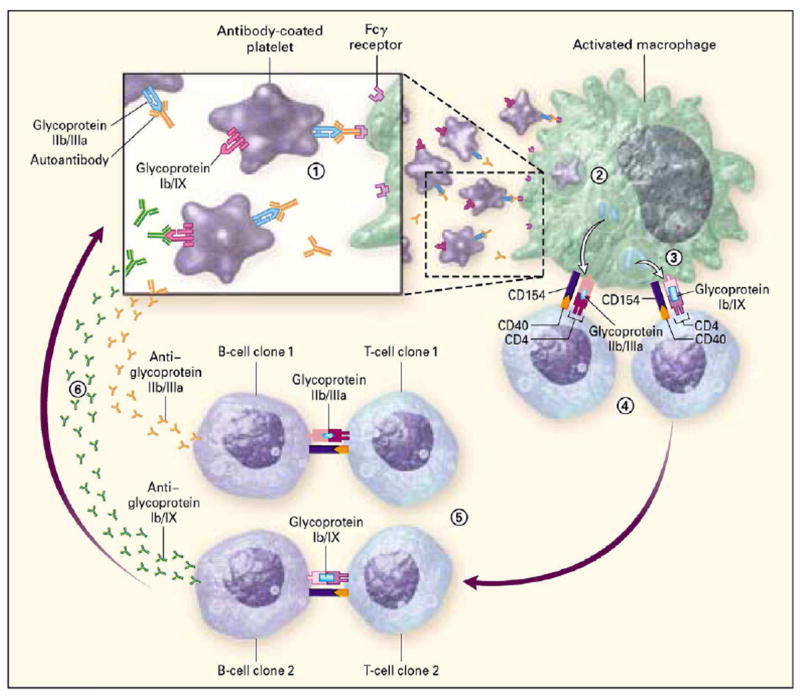
The factors that initiate autoantibody production are unknown. Many patients have antibodies against several platelet surface glycoproteins at the time the disease becomes clinically evident. Here, glycoprotein IIb/IIIa is recognized by autoantibody (orange, inset), whereas antibodies that recognize the glycoprotein Ib/IX complex have not been generated at this stage (1). Antibody-coated platelets bind to antigen presenting cells (macrophages or dendritic cells) through Fcγ receptors and are then internalized and degraded (2). Antigen presenting cells not only degrade glycoprotein IIb/IIIa (light blue oval), thereby amplifying the initial immune response, but also may generate cryptic epitopes from other platelet glycoproteins (light blue cylinder) (3). Activated antigen-presenting cells (4) express these novel peptides on the cell surface along with costimulatory help (represented in part by the interaction between CD154 and CD40) and the relevant cytokines that facilitate the proliferation of the initiating CD4-positive T-cell clones (T-cell clone 1) and those with additional specificities (T-cell clone 2) (5). B-cell immunoglobulin receptors that recognize additional platelet antigens (B-cell clone 2) are thereby also induced to proliferate and synthesize anti-glycoprotein Ib/IX antibodies (green) in addition to amplifying the production of anti-glycoprotein IIb/IIIa antibodies (orange) by B-cell clone 1 (6). From Cines DB, Blanchette VS. Immune thrombocytopenic purpura. N Engl J Med 2002;346:13-995, with permission.
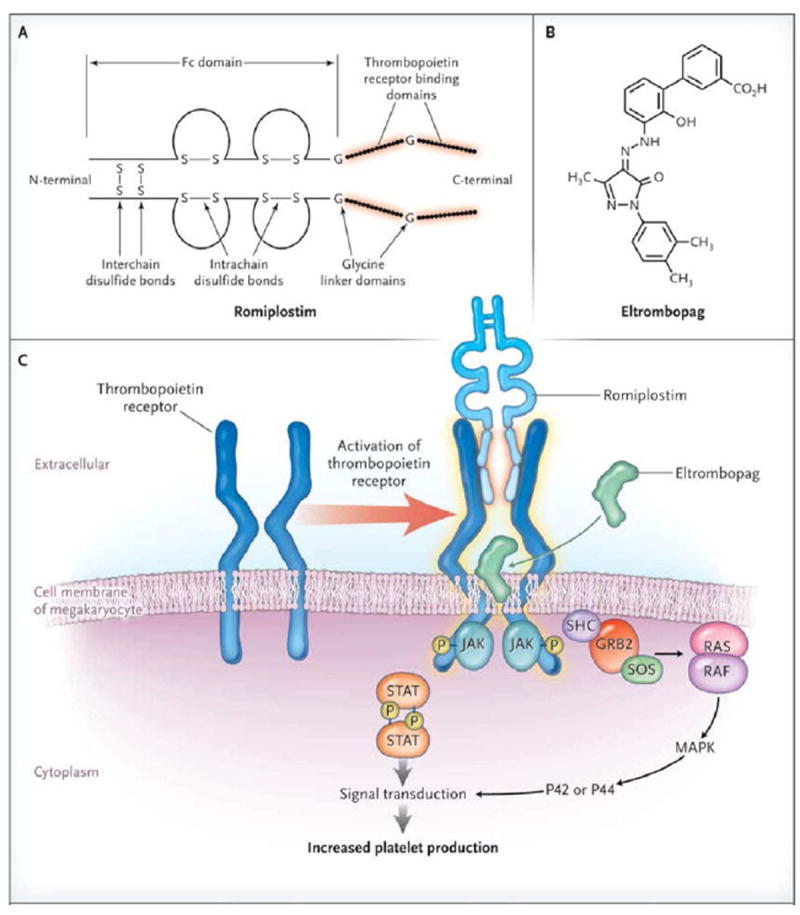
Panel A shows the chemical structure of romiplostim, which is composed of the Fc portion of IgG1, to which two thrombopoietin peptides consisting of 14 amino acids are coupled through glycine bridges at the C-terminal of each γ heavy chain. Panel B shows the chemical structure of eltrombopag. Panel C shows the cellular mechanisms of action of romiplostim, which binds to the thrombopoietin receptor, and of eltrombopag, which binds to the thrombopoietin receptor’s transmembrane domain, thereby activating signaling that leads to increased platelet production. GRB2 denotes growth factor receptor-binding protein 2, JAK Janus kinase, MAPK mitogen-activated protein kinase, P phosphorylation, RAF rapidly accelerated fibrosarcoma kinase, RAS rat sarcoma GTPase, SHC Src homology collagen protein, and STAT signal transducer and activator of transcription. From Imbach P, Crowther M. Thrombopoietin-receptor agonists for primary immune thrombocytopenia. N Engl J Med 2011;365(8):734-741, with permission.
References
-
- Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113:2386–2393. - PubMed
-
- Stasi R, Newland AC. ITP: a historical perspective. Br J Haematol. 2011;153(4):437–450. - PubMed
-
- Cuker A, Cines DB. Immune thrombocytopenia. Hematology Am Soc Hematol Educ Program. 2010;2010:377–84. - PubMed
-
- Semple JW, Provan D, Garvey MB, Freedman J. Recent progress in understanding the pathogenesis of immune thrombocytopenia. Curr Opin Hematol. 2010;17(6):590–595. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
