

Clinico-biological features of 5202 patients with acute lymphoblastic leukemia enrolled in the Italian AIEOP and GIMEMA protocols and stratified in age cohorts
- PMID: 23716539
- PMCID: PMC3815170
- DOI: 10.3324/haematol.2012.080432
Clinico-biological features of 5202 patients with acute lymphoblastic leukemia enrolled in the Italian AIEOP and GIMEMA protocols and stratified in age cohorts
Abstract
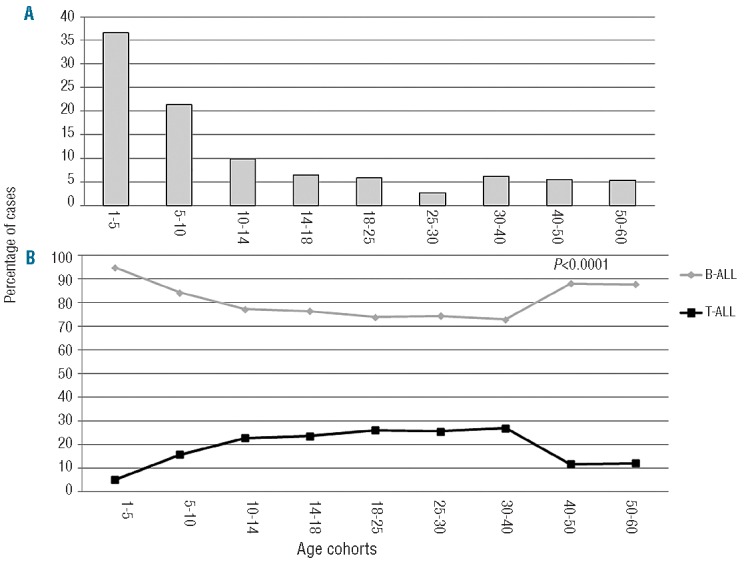
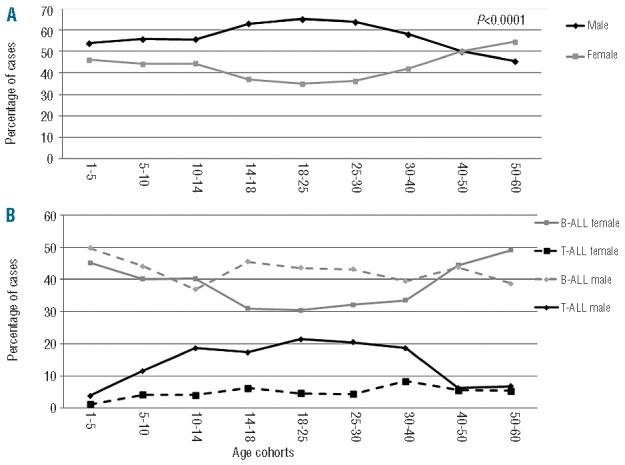
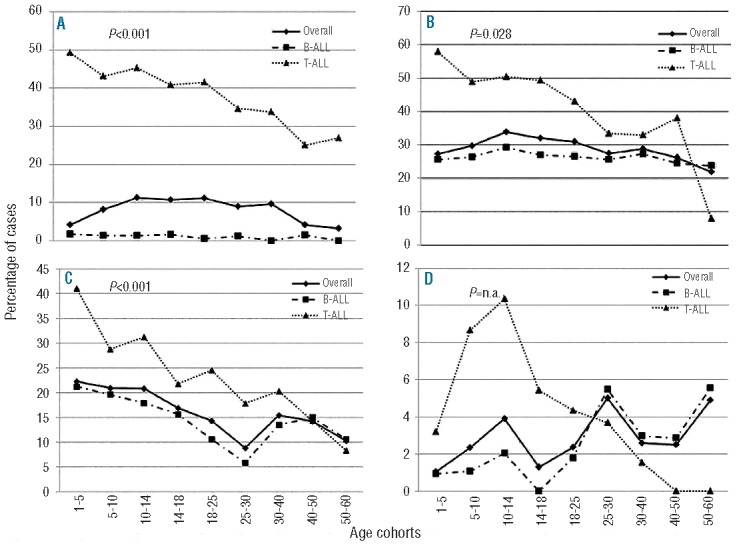
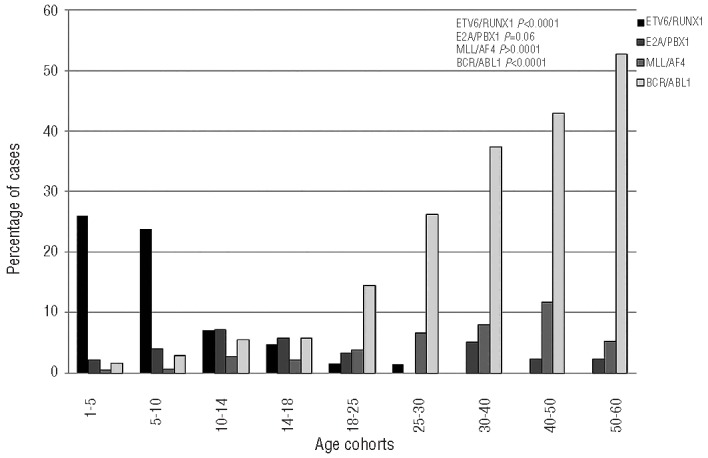
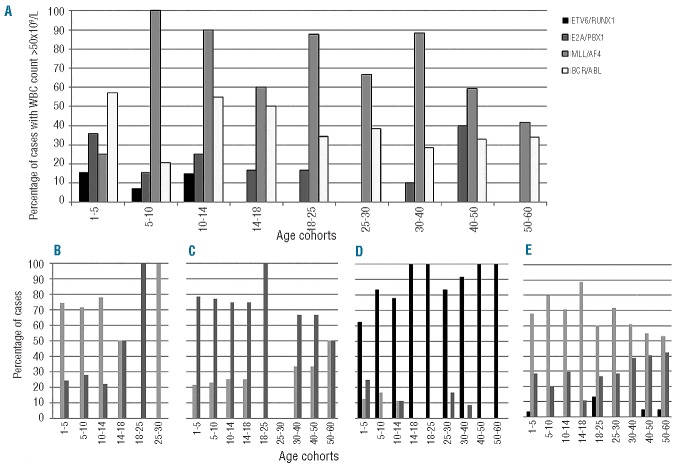
The outcome of children and adults with acute lymphoblastic leukemia is markedly different. Since there is limited information on the distribution of clinico-biological variables in different age cohorts, we analyzed 5202 patients with acute lymphoblastic leukemia enrolled in the Italian multicenter AIEOP and GIMEMA protocols and stratified them in nine age cohorts. The highest prevalence of acute lymphoblastic leukemia was observed in children, although a second peak was recorded from the 4(th) decade onwards. Interestingly, the lowest incidence was found in females between 14-40 years. Immunophenotypic characterization showed a B-lineage in 85.8% of patients: a pro-B stage, associated with MLL/AF4 positivity, was more frequent in patients between 10-50 years. T-lineage leukemia (14.2%) was rare among small children and increased in patients aged 10-40 years. The prevalence of the BCR/ABL1 rearrangement increased progressively with age starting from the cohort of patients 10-14 years old and was present in 52.7% of cases in the 6th decade. Similarly, the MLL/AF4 rearrangement constantly increased up to the 5(th) decade, while the ETV6/RUNX1 rearrangement disappeared from the age of 30 onwards. This study shows that acute lymphoblastic leukemia in adolescents and young adults is characterized by a male prevalence, higher percentage of T-lineage cases, an increase of poor prognostic molecular markers with aging compared to cases in children, and conclusively quantified the progressive increase of BCR/ABL(+) cases with age, which are potentially manageable by targeted therapies.
Figures
References
-
- Silverman LB, Gelber RD, Dalton VK, Asselin BL, Barr RD, Clavell LA, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97(5):1211–8 - PubMed
-
- Pui CH, Robison LL, Look AT. Acute lymphoblastic leukaemia. Lancet. 2008;371 (9617):1030–43 - PubMed
-
- Annino L, Vegna ML, Camera A, Specchia G, Visani G, Fioritoni G, et al. Treatment of adult acute lymphoblastic leukemia (ALL): long-term follow-up of the GIMEMA ALL 0288 randomized study. Blood. 2002;99 (3):863–71 - PubMed
-
- Rowe JM, Buck G, Burnett AK, Chopra R, Wiernik PH, Richards SM, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106 (12):3760–7 - PubMed
-
- Thomas X, Boiron JM, Huguet F, Dombret H, Bradstock K, Vey N, et al. Outcome of treatment in adults with acute lymphoblastic leukemia: analysis of the LALA-94 trial. J Clin Oncol. 2004;22(20):4075–8 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
