

Surgical outcomes in phacoemulsification after application of a risk stratification system
- PMID: 23717035
- PMCID: PMC3663436
- DOI: 10.2147/OPTH.S42726
Surgical outcomes in phacoemulsification after application of a risk stratification system
Abstract
Background: The purpose of this study was to determine whether application of a risk stratification system during preoperative assessment of cataract patients and subsequent allocation of patients to surgeons with matching experience may reduce intraoperative complications.
Methods: Nine hundred and fifty-three consecutive patients (1109 eyes) undergoing phacoemulsification cataract surgery were assigned to two groups, ie, group A (n = 498 patients, 578 eyes) and group B (n = 455 patients, 531 eyes). Patients from group A were allocated to surgeons with varying experience with only a rough estimate of the complexity of their surgery. Patients from group B were assigned to three risk groups (no added risk, low risk, and moderate-high risk) according to risk factors established during their preoperative assessment and were respectively allocated to resident surgeons, low-volume surgeons, or high-volume surgeons. Data were collected and entered into a computerized database. The intraoperative complication rate was calculated for each group.
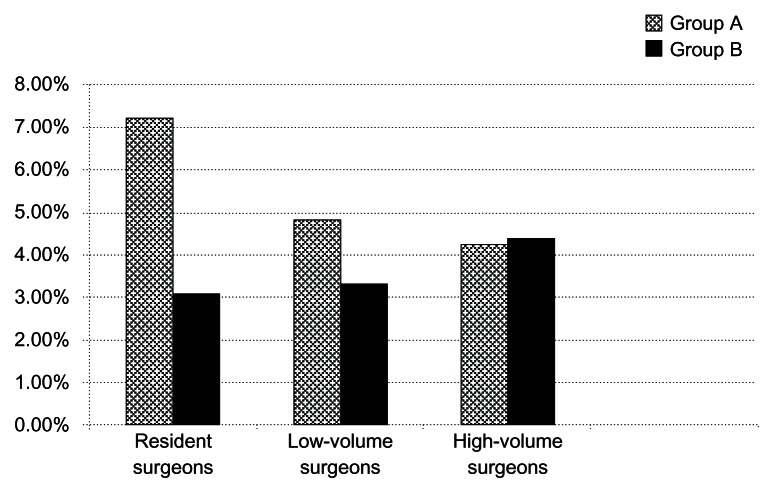
Results: The intraoperative complication rate was significantly lower in group B than in group A (group A, 5.88%; group B, 3.2%; P < 0.05). Patients from group B with no added risk and allocated to resident surgeons had a significantly lower rate of intraoperative complications than those from group A allocated to resident surgeons (group A, 7.2%; group B, 3.08%; P < 0.05).
Conclusion: Our study demonstrates that allocation of cataract patients to surgeons matched for experience according to a uniform and reliable preoperative assessment of their risk of complications allows for better surgical outcomes, especially for resident surgeons.
Keywords: cataract; complications; resident; risk stratification.
Figures
References
-
- Tabin G, Chen M, Espandar L. Cataract surgery for the developing world. Curr Opin Ophthalmol. 2008;19(1):55–59. - PubMed
-
- Qatarneh D, Mathew RG, Palmer S, Bunce C, Tuft S. The economic cost of posterior capsule tear at cataract surgery. Br J Ophthalmol. 2012;96(1):114–117. - PubMed
-
- Malot J, Combe C, Savary P, Moss A, Ligeon-Ligeonnet P, Hida H. Direct cost of cataract surgery in public hospitals. Ann Pharm Fr. 2010;68(6):380–387. French. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
