

Computed tomography-based diagnostics might be insufficient in the determination of pancreatic cancer unresectability
- PMID: 23717744
- PMCID: PMC3664295
- DOI: 10.4240/wjgs.v5.i4.83
Computed tomography-based diagnostics might be insufficient in the determination of pancreatic cancer unresectability
Abstract
Aim: To inquire into a question of an overestimation of arterial involvement in patients with pancreatic cancer (PC).
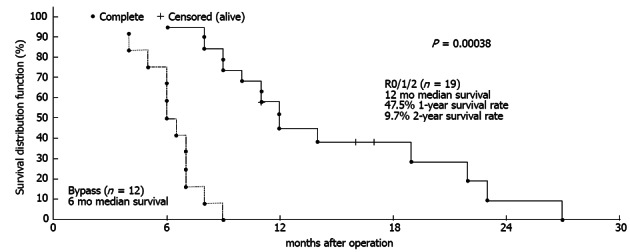
Methods: Radiology data were compared with the findings from 51 standard, 58 extended and 17 total pancreaticoduodenectomies; 9 distal resections with celiac artery (CA) excision; and 28 palliations for PC. The survival of 11 patients with controversial computed tomography (CT) and endoscopic ultrasound data with regard to arterial invasion, after R0/R1 procedures (false-positive CT results, Group A), was compared to survival after eight R2 resections (false-negative CT results, Group B) and after 12 bypass procedures for locally advanced cancer (true-positive CT results, Group C).
Results: In all of the cases in group A, operative exploration revealed no arterial invasion, which was predicted by CT. The one-year survival in Group A was 88.9%, and the two-year survival was 26.7%, with a median follow-up of 22 mo. One-year survival was not attained in groups B and C, with a significant difference in survival (P a-b = 0.0029, P b-c = 0.003).
Conclusion: Arterial encasement on CT does not necessarily indicate arterial invasion. Whenever PC is considered unresectable, endoUS should be used. In patients with controversial CT an EUS data for peripancreatic arteries involvement radical resection might be possible, providing survival benefits as compared to R2- resections or palliative surgery.
Keywords: Arteries; Cancer; Computed tomography; Distal pancreatectomy; Endoscopic ultrasound; Management; Pancreas; Pancreaticoduodenectomy; Resectability; Vascular invasion.
Figures






References
-
- Hackert T, Büchler MW, Werner J. Surgical management of pancreatic cancer-standard and extended resections. Eur Surg. 2009;41:293–299.
-
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011;61:212–236. - PubMed
-
- Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, editors. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010. pp. 241–249.
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Pancreatic Adenocarcinoma Version 2. Fort Washington, PA: National Comprehensive Cancer Network, Inc (NCCN); 2012.
LinkOut - more resources
Full Text Sources
Other Literature Sources
