

Imaging of brain metastases
- PMID: 23717792
- PMCID: PMC3656556
- DOI: 10.4103/2152-7806.111298
Imaging of brain metastases
Abstract
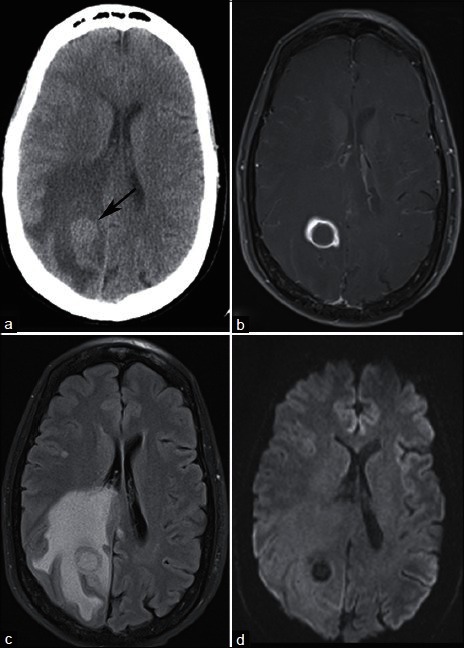
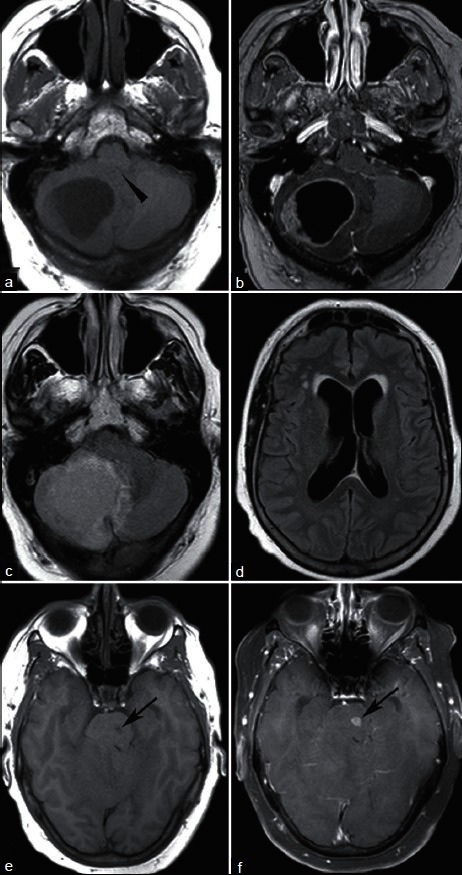
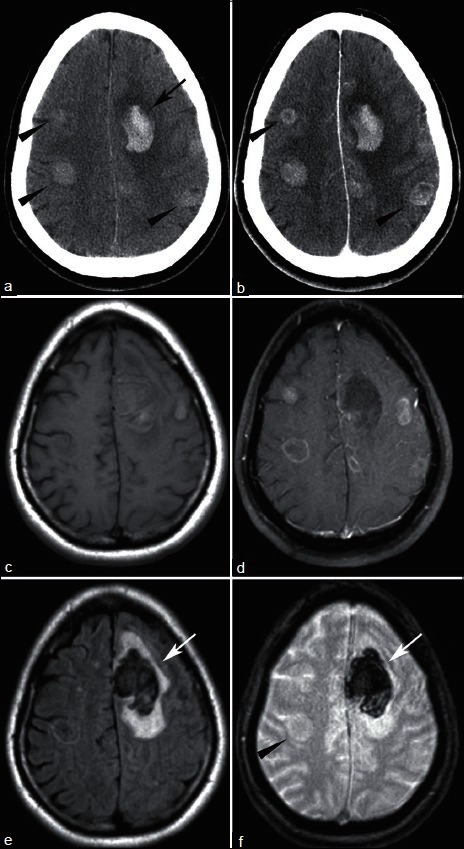
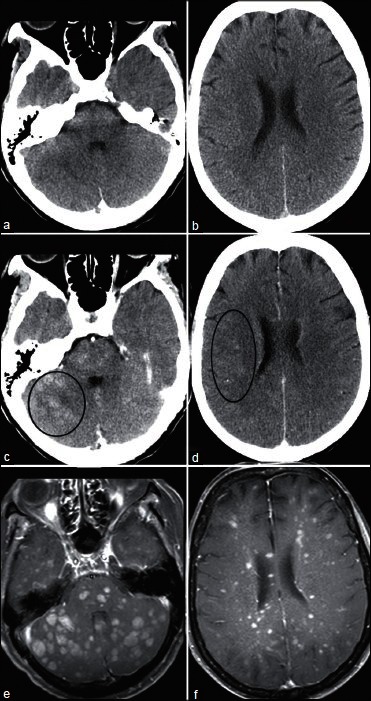
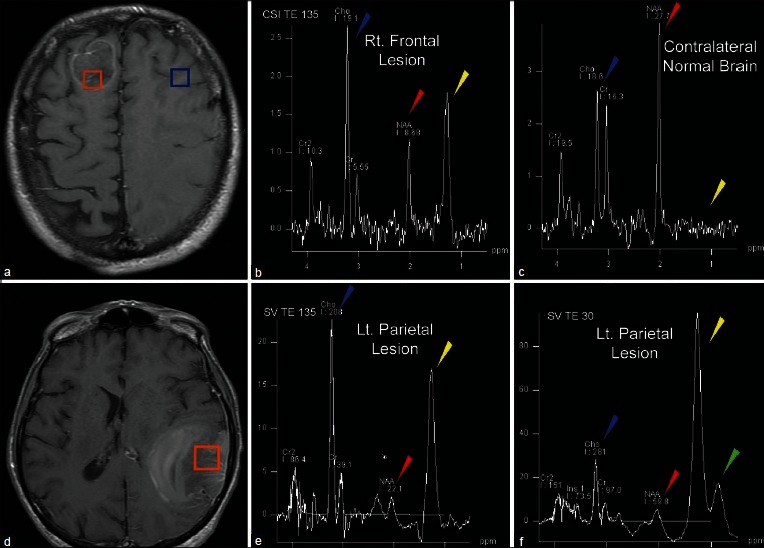
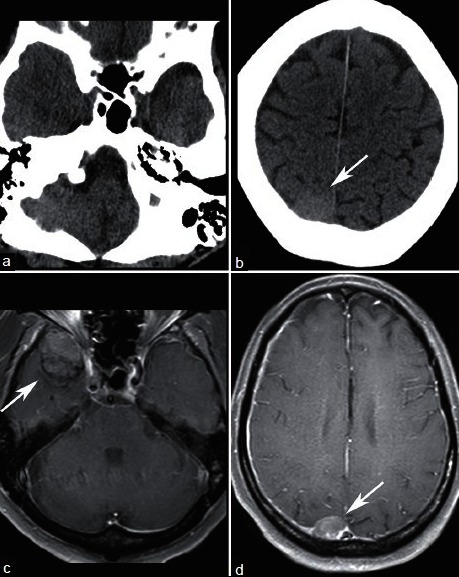
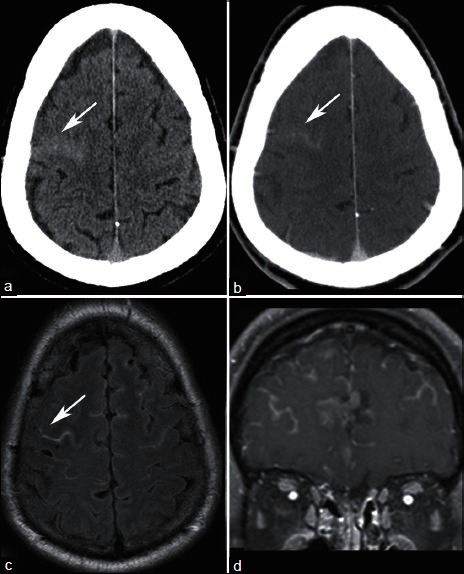
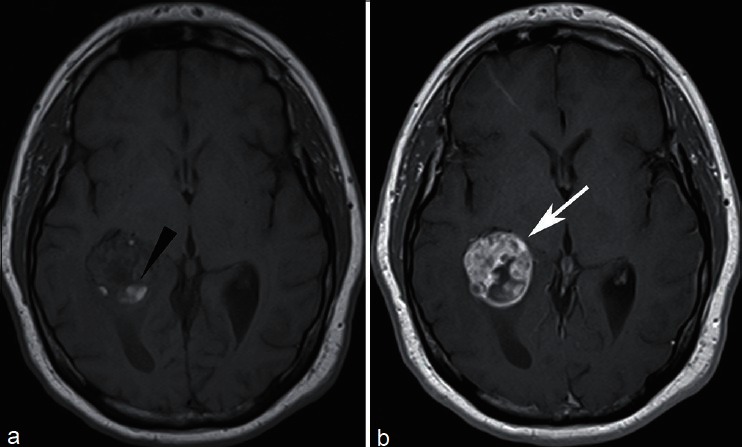
Imaging plays a key role in the diagnosis of central nervous system (CNS) metastasis. Imaging is used to detect metastases in patients with known malignancies and new neurological signs or symptoms, as well as to screen for CNS involvement in patients with known cancer. Computed tomography (CT) and magnetic resonance imaging (MRI) are the key imaging modalities used in the diagnosis of brain metastases. In difficult cases, such as newly diagnosed solitary enhancing brain lesions in patients without known malignancy, advanced imaging techniques including proton magnetic resonance spectroscopy (MRS), contrast enhanced magnetic resonance perfusion (MRP), diffusion weighted imaging (DWI), and diffusion tensor imaging (DTI) may aid in arriving at the correct diagnosis. This image-rich review discusses the imaging evaluation of patients with suspected intracranial involvement and malignancy, describes typical imaging findings of parenchymal brain metastasis on CT and MRI, and provides clues to specific histological diagnoses such as the presence of hemorrhage. Additionally, the role of advanced imaging techniques is reviewed, specifically in the context of differentiating metastasis from high-grade glioma and other solitary enhancing brain lesions. Extra-axial CNS involvement by metastases, including pachymeningeal and leptomeningeal metastases is also briefly reviewed.
Keywords: Brain metastasis; computed tomography; diffusion weighted imaging; magnetic resonance imaging; magnetic resonance perfusion; magnetic resonance spectroscopy.
Figures
References
-
- Atlas SW, Atlas SW, editors. 4th ed. Vol. 2. Philadelphia: Wolters Kluwer Health/Lippincott Williams and Wilkins; 2009. Magnetic Resonance Imaging of the Brain and Spine.
-
- Akeson P, Larsson EM, Kristoffersen DT, Jonsson E, Holtås S. Brain metastases-comparison of gadodiamide injection-enhanced MR imaging at standard and high dose, contrast-enhanced CT and non-contrast-enhanced MR imaging. Acta Radiol. 1995;36:300–6. - PubMed
-
- Al-Okaili RN, Krejza J, Wang S, Woo JH, Melhem ER. Advanced MR imaging techniques in the diagnosis of intraaxial brain tumors in adults. Radiographics. 2006;26(Suppl 1):S173–89. - PubMed
-
- Balériaux D, Colosimo C, Ruscalleda J, Korves M, Schneider G, Bohndorf K, et al. Magnetic resonance imaging of metastatic disease to the brain with gadobenate dimeglumine. Neuroradiology. 2002;44:191–203. - PubMed
-
- Barajas RF, Cha S. Imaging diagnosis of brain metastasis. Prog Neurol Surg. 2012;25:55–73. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
