

Targeted versus universal decolonization to prevent ICU infection
- PMID: 23718152
- PMCID: PMC10853913
- DOI: 10.1056/NEJMoa1207290
Targeted versus universal decolonization to prevent ICU infection
Erratum in
- N Engl J Med. 2013 Aug 8;369(6):587
- N Engl J Med. 2014 Feb 27;370(9):886
Abstract
Background: Both targeted decolonization and universal decolonization of patients in intensive care units (ICUs) are candidate strategies to prevent health care-associated infections, particularly those caused by methicillin-resistant Staphylococcus aureus (MRSA).
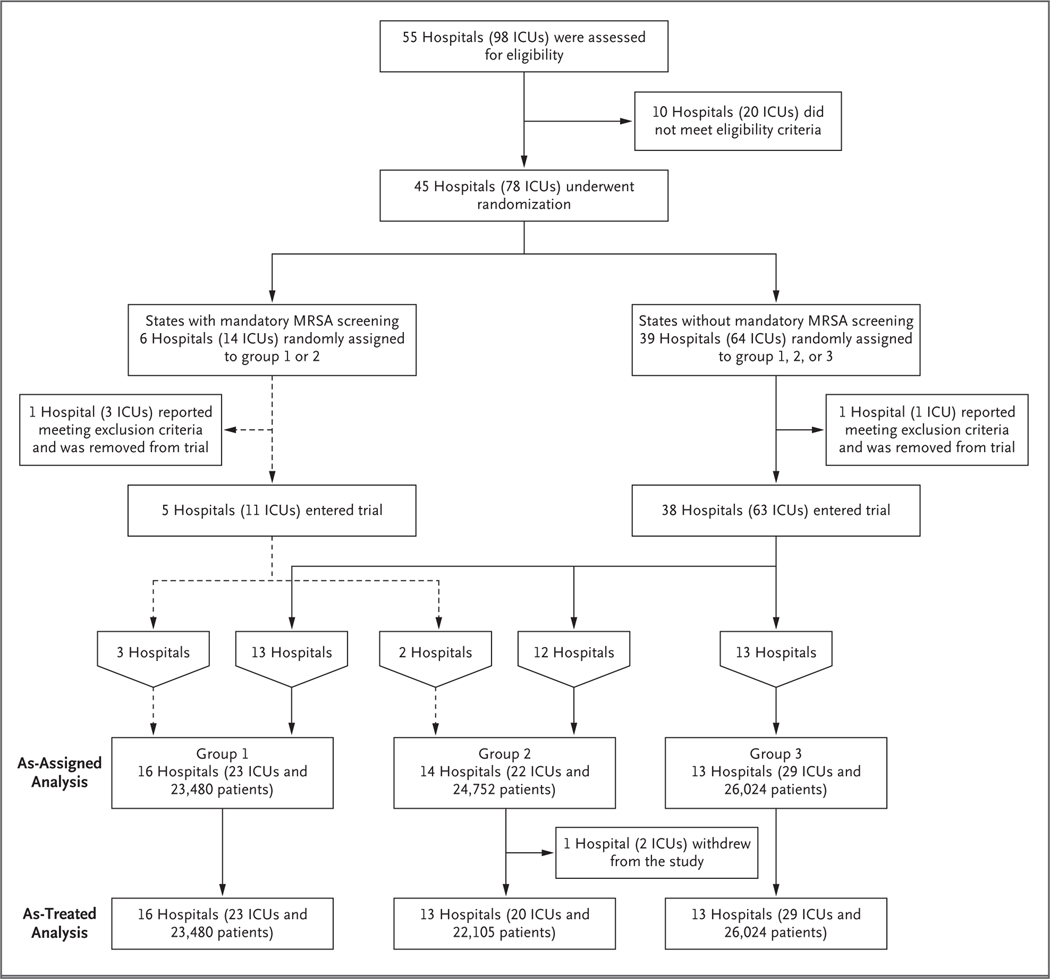
Methods: We conducted a pragmatic, cluster-randomized trial. Hospitals were randomly assigned to one of three strategies, with all adult ICUs in a given hospital assigned to the same strategy. Group 1 implemented MRSA screening and isolation; group 2, targeted decolonization (i.e., screening, isolation, and decolonization of MRSA carriers); and group 3, universal decolonization (i.e., no screening, and decolonization of all patients). Proportional-hazards models were used to assess differences in infection reductions across the study groups, with clustering according to hospital.
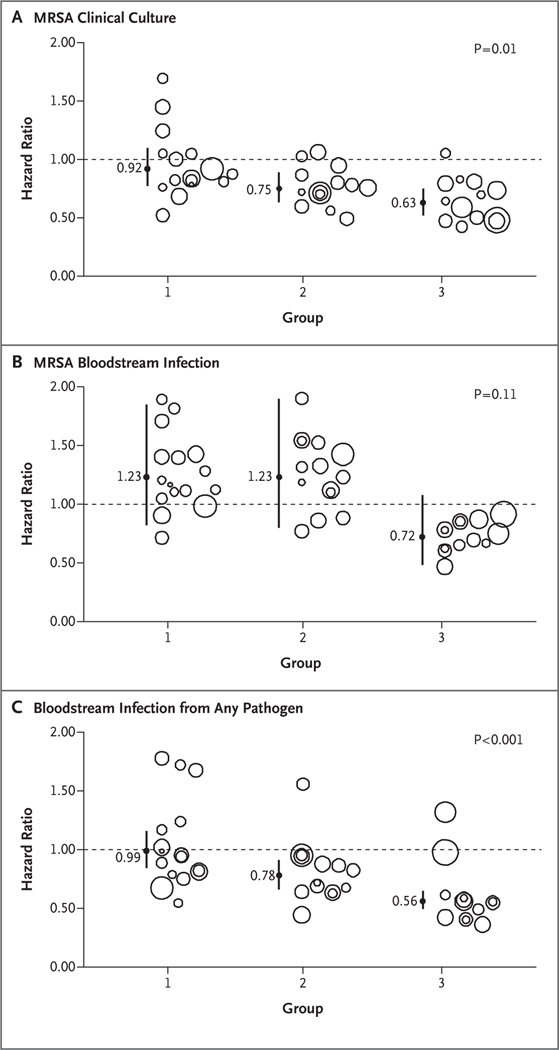
Results: A total of 43 hospitals (including 74 ICUs and 74,256 patients during the intervention period) underwent randomization. In the intervention period versus the baseline period, modeled hazard ratios for MRSA clinical isolates were 0.92 for screening and isolation (crude rate, 3.2 vs. 3.4 isolates per 1000 days), 0.75 for targeted decolonization (3.2 vs. 4.3 isolates per 1000 days), and 0.63 for universal decolonization (2.1 vs. 3.4 isolates per 1000 days) (P=0.01 for test of all groups being equal). In the intervention versus baseline periods, hazard ratios for bloodstream infection with any pathogen in the three groups were 0.99 (crude rate, 4.1 vs. 4.2 infections per 1000 days), 0.78 (3.7 vs. 4.8 infections per 1000 days), and 0.56 (3.6 vs. 6.1 infections per 1000 days), respectively (P<0.001 for test of all groups being equal). Universal decolonization resulted in a significantly greater reduction in the rate of all bloodstream infections than either targeted decolonization or screening and isolation. One bloodstream infection was prevented per 54 patients who underwent decolonization. The reductions in rates of MRSA bloodstream infection were similar to those of all bloodstream infections, but the difference was not significant. Adverse events, which occurred in 7 patients, were mild and related to chlorhexidine.
Conclusions: In routine ICU practice, universal decolonization was more effective than targeted decolonization or screening and isolation in reducing rates of MRSA clinical isolates and bloodstream infection from any pathogen. (Funded by the Agency for Healthcare Research and the Centers for Disease Control and Prevention; REDUCE MRSA ClinicalTrials.gov number, NCT00980980).
Figures
Comment in
-
Screening inpatients for MRSA--case closed.N Engl J Med. 2013 Jun 13;368(24):2314-5. doi: 10.1056/NEJMe1304831. Epub 2013 May 29. N Engl J Med. 2013. PMID: 23718155 No abstract available.
-
Universal decolonization was better than MRSA screening and isolation for preventing nosocomial ICU infections.Ann Intern Med. 2013 Sep 17;159(6):JC4. doi: 10.7326/0003-4819-159-6-201309170-02004. Ann Intern Med. 2013. PMID: 24042387 No abstract available.
-
Targeted decolonization to prevent ICU infections.N Engl J Med. 2013 Oct 10;369(15):1470-1. doi: 10.1056/NEJMc1309704. N Engl J Med. 2013. PMID: 24106942 No abstract available.
-
Targeted decolonization to prevent ICU infections.N Engl J Med. 2013 Oct 10;369(15):1468. doi: 10.1056/NEJMc1309704. N Engl J Med. 2013. PMID: 24106943 No abstract available.
-
Targeted decolonization to prevent ICU infections.N Engl J Med. 2013 Oct 10;369(15):1468-9. doi: 10.1056/NEJMc1309704. N Engl J Med. 2013. PMID: 24106944 No abstract available.
-
Targeted decolonization to prevent ICU infections.N Engl J Med. 2013 Oct 10;369(15):1469. doi: 10.1056/NEJMc1309704. N Engl J Med. 2013. PMID: 24106945 No abstract available.
-
Targeted decolonization to prevent ICU infections.N Engl J Med. 2013 Oct 10;369(15):1469-70. doi: 10.1056/NEJMc1309704. N Engl J Med. 2013. PMID: 24106946 No abstract available.
-
[Decolonization to prevent infections in the ICU].Rev Chilena Infectol. 2013 Oct;30(5):571. doi: 10.4067/S0716-10182013000500018. Rev Chilena Infectol. 2013. PMID: 24248176 Spanish. No abstract available.
-
Preventing infection in the intensive care unit: targeted or universal decolonization.Natl Med J India. 2013 May-Jun;26(3):161-3. Natl Med J India. 2013. PMID: 24476164 No abstract available.
-
[Prevention of catheter-related sepsis].Med Klin Intensivmed Notfmed. 2014 May;109(4):225. Med Klin Intensivmed Notfmed. 2014. PMID: 24936635 German. No abstract available.
-
Universal decolonization to prevent intensive care unit meticillin-resistant Staphylococcus aureus infection.J Hosp Infect. 2014 Nov;88(3):179-80. doi: 10.1016/j.jhin.2014.08.003. Epub 2014 Aug 28. J Hosp Infect. 2014. PMID: 25228226 No abstract available.
References
-
- Jarvis WR, Jarvis AA, Chinn RY. National prevalence of methicillin-resistant Staphylococcus aureus in inpatients at US health care facilities, 2010. Am J Infect Control 2012;40:194–200. - PubMed
-
- Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA 2007;298:1763–71. - PubMed
-
- Sievert DM, Ricks P, Edwards JR, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Control Hosp Epidemiol 2013;34:1–14. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical