

Health outcomes of HIV-exposed uninfected African infants
- PMID: 23719347
- PMCID: PMC4493890
- DOI: 10.1097/QAD.0b013e32835ca29f
Health outcomes of HIV-exposed uninfected African infants
Abstract
Objectives: To evaluate severe (grade 3/4) morbidity and mortality in HIV-exposed, uninfected infants.
Design: : Secondary data analysis of The Breastfeeding, Antiretrovirals, and Nutrition (BAN) clinical trial.
Methods: BAN randomized 2369 mother-infant pairs to maternal, infant, or no extended antiretroviral prophylaxis during breastfeeding. Morbidity outcomes examined were pneumonia/serious febrile illness, diarrhea/growth faltering, and malaria. Infant death was defined as neonatal (≤30 days of life), and postneonatal (31 days to 48 weeks of life). Cox proportional hazards models were used to evaluate the effect of covariates on infant morbidity and mortality.
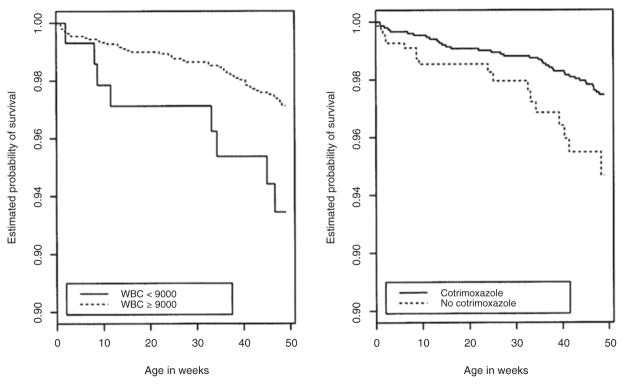
Results: The rate of pneumonia/serious febrile illness was highest in the first 12 weeks (0.83/100 person-weeks) before rapidly decreasing; rates of all morbidity outcomes increased after 24 weeks. Rates of pneumonia/serious febrile illness and diarrhea/growth faltering were higher during the rainy season. Prophylactic infant cotrimoxazole significantly decreased the rates of all morbidity outcomes. White blood cell (WBC) count less than 9000/μl at birth was associated with increased diarrhea/growth faltering [adjusted hazard ratio (aHR) 1.73, P = 0.04] and malaria (aHR 2.18, P = 0.02). Low birth weight (2000-2499 g) was associated with neonatal death (aHR 12.3, P < 0.001). Factors associated with postneonatal death included rainy season (aHR 4.24, P = 0.002), infant cotrimoxazole (aHR 0.48, P = 0.03), and low infant WBC count at birth (aHR 2.53, P = 0.02).
Conclusion: Infant morbidity rates increased after 24 weeks, when BAN infants weaned. Introduction of prophylactic cotrimoxazole was associated with reduced rates of morbidity and mortality in HIV-exposed uninfected infants. Unexpectedly, a low WBC count at birth was significantly associated with later infant morbidity and mortality in this cohort.
Conflict of interest statement
The University of North Carolina received grant support from Abbott Laboratories and GlaxoSmithKline. M.H. has received lecture fees from Abbott. All other authors declare that they have no conflicts of interest.
Figures
References
-
- WHO. Rapid advice: use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Geneva, Switzerland: WHO; 2009.
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F, et al. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364:1236–1243. - PubMed
-
- Brahmbhatt H, Kigozi G, Wabwire-Mangen F, Serwadda D, Lutalo T, Nalugoda F, et al. Mortality in HIV-infected and uninfected children of HIV-infected and uninfected mothers in rural Uganda. J Acquir Immune Defic Syndr. 2006;41:504–508. - PubMed
-
- Koyanagi A, Humphrey JH, Ntozini R, Nathoo K, Moulton LH, Iliff P, et al. Morbidity among human immunodeficiency virus-exposed but uninfected, human immunodeficiency virus-infected, and human immunodeficiency virus-unexposed infants in Zimbabwe before availability of highly active anti-retroviral therapy. Pediatr Infect Dis J. 2011;30:45–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
