

Cognitive and emotional control of pain and its disruption in chronic pain
- PMID: 23719569
- PMCID: PMC4465351
- DOI: 10.1038/nrn3516
Cognitive and emotional control of pain and its disruption in chronic pain
Abstract
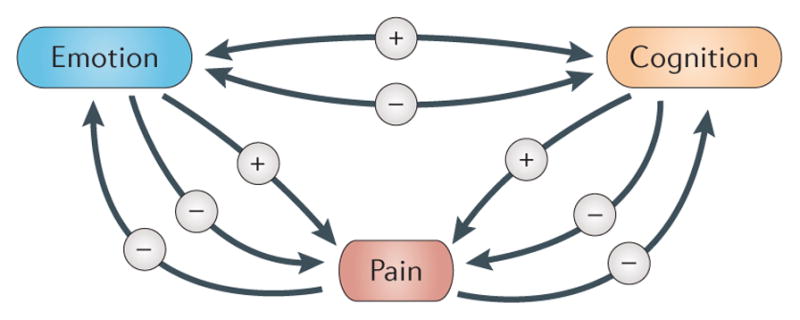
Chronic pain is one of the most prevalent health problems in our modern world, with millions of people debilitated by conditions such as back pain, headache and arthritis. To address this growing problem, many people are turning to mind-body therapies, including meditation, yoga and cognitive behavioural therapy. This article will review the neural mechanisms underlying the modulation of pain by cognitive and emotional states - important components of mind-body therapies. It will also examine the accumulating evidence that chronic pain itself alters brain circuitry, including that involved in endogenous pain control, suggesting that controlling pain becomes increasingly difficult as pain becomes chronic.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Bingel U, et al. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med. 2011;3:70ra14. - PubMed
-
- Villemure C, Bushnell MC. Cognitive modulation of pain: how do attention and emotion influence pain processing? Pain. 2002;95:195–199. - PubMed
-
- Loggia ML, Mogil JS, Bushnell MC. Empathy hurts: compassion for another increases both sensory and affective components of pain perception. Pain. 2008;136:168–176. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
