

Twenty-four hour non-invasive ambulatory blood pressure and heart rate monitoring in Parkinson's disease
- PMID: 23720648
- PMCID: PMC3654335
- DOI: 10.3389/fneur.2013.00049
Twenty-four hour non-invasive ambulatory blood pressure and heart rate monitoring in Parkinson's disease
Abstract
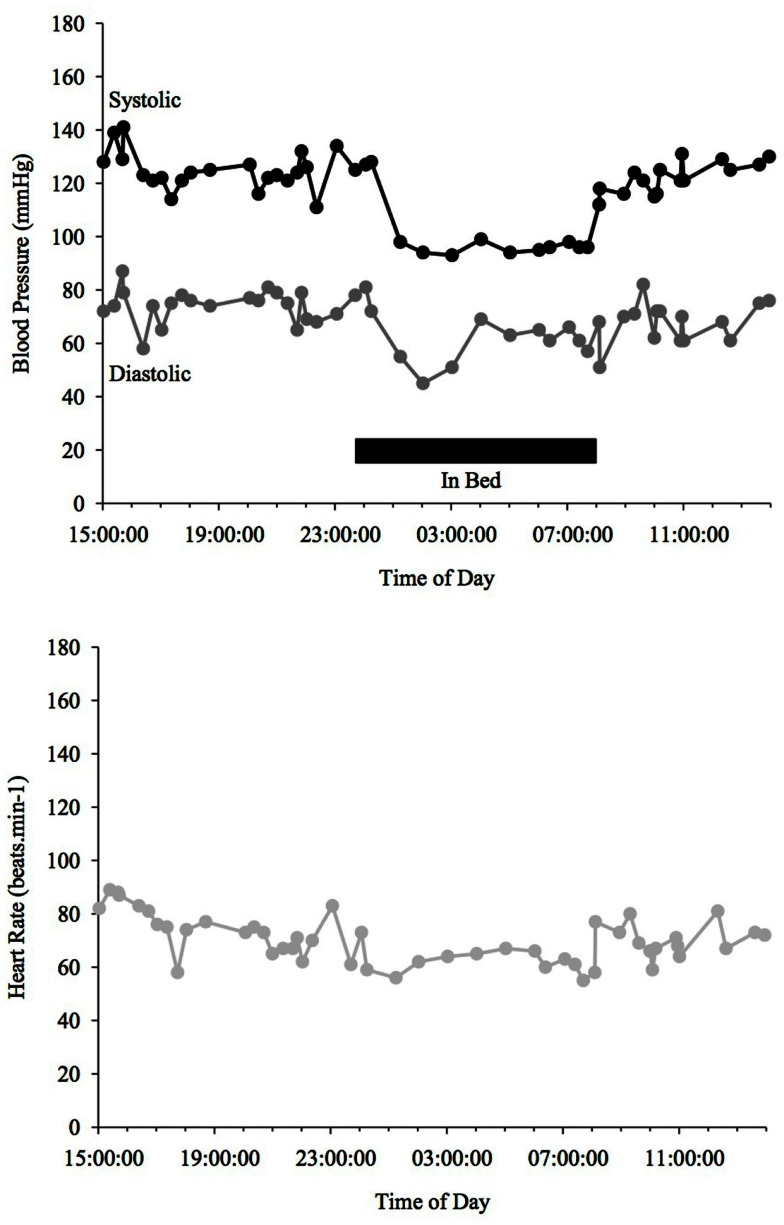
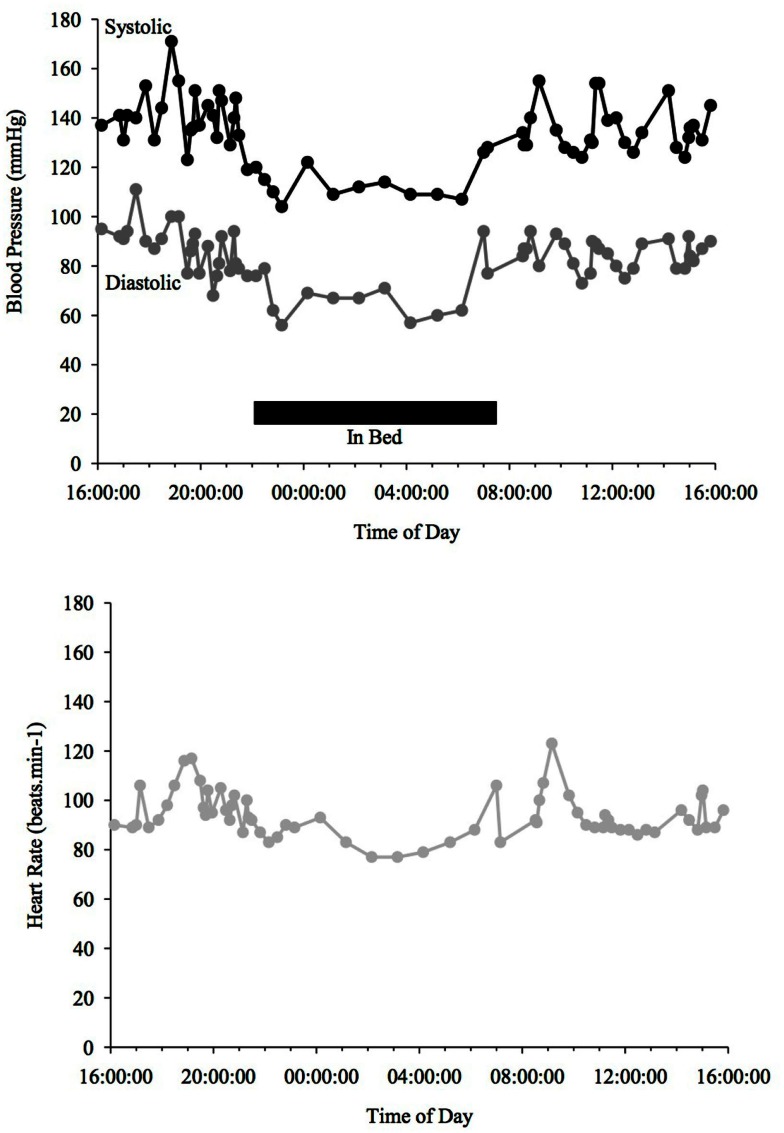
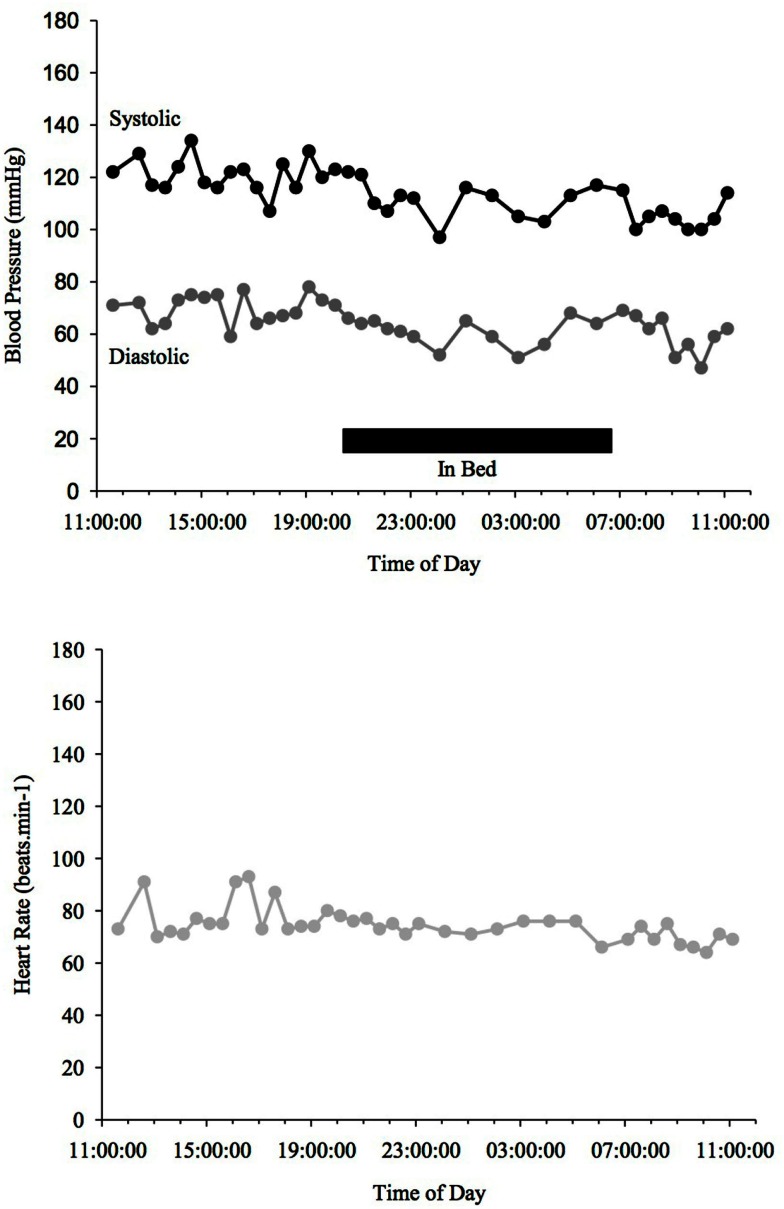
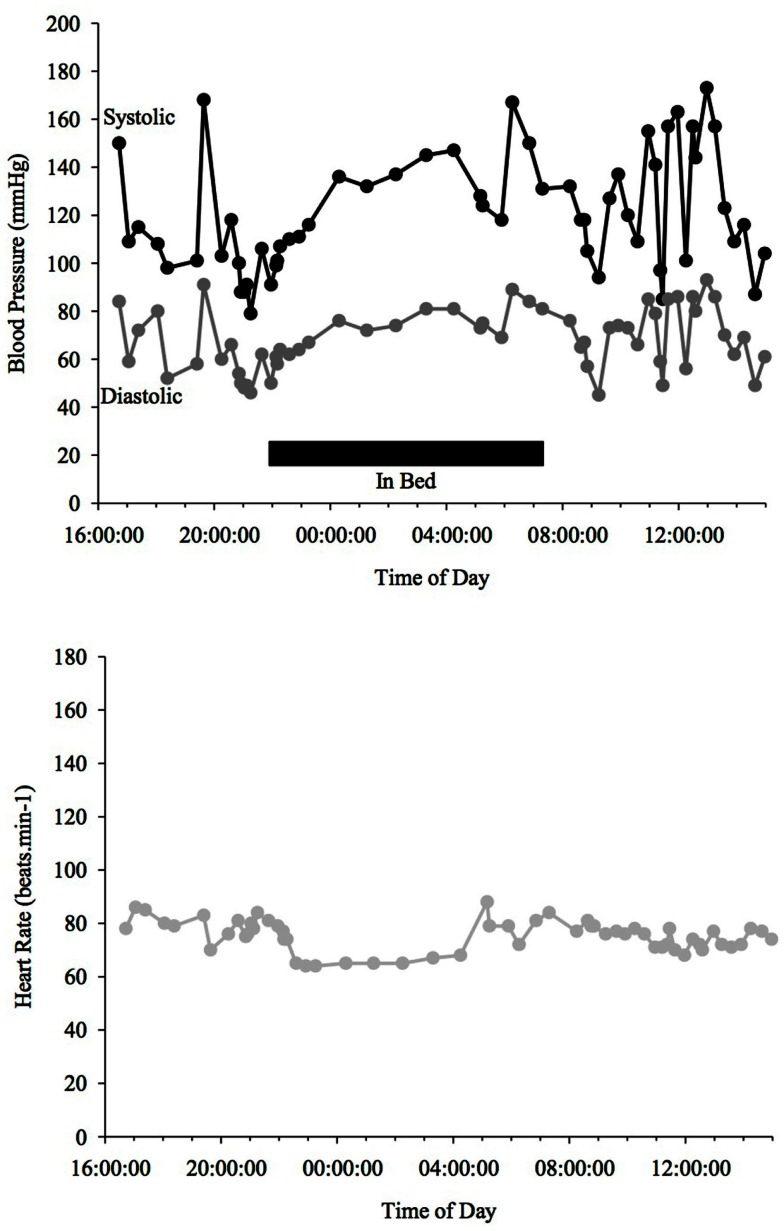
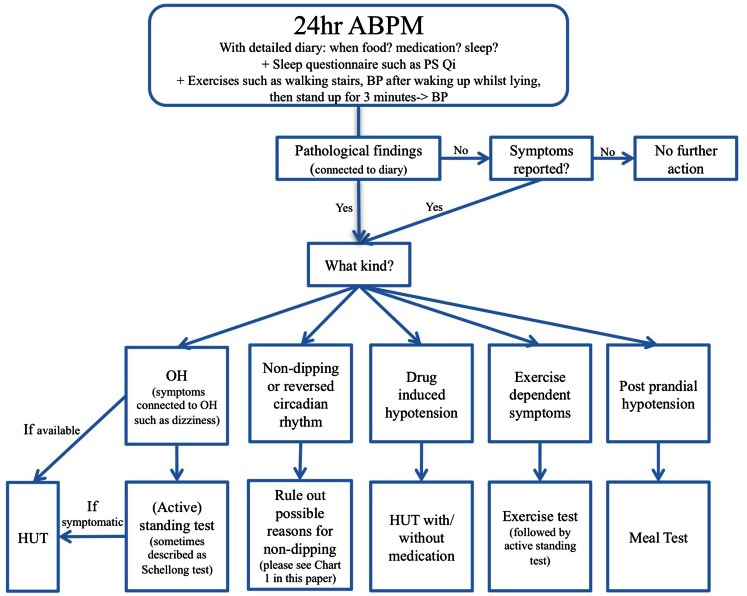
Non-motor symptoms are now commonly recognized in Parkinson's disease (PD) and can include dysautonomia. Impairment of cardiovascular autonomic function can occur at any stage of PD but is typically prevalent in advanced stages or related to (anti-Parkinsonian) drugs and can result in atypical blood pressure (BP) readings and related symptoms such as orthostatic hypotension (OH) and supine hypertension. OH is usually diagnosed with a head-up-tilt test (HUT) or an (active) standing test (also known as Schellong test) in the laboratory, but 24 h ambulatory blood pressure monitoring (ABPM) in a home setting may have several advantages, such as providing an overview of symptoms in daily life alongside pathophysiology as well as assessment of treatment interventions. This, however, is only possible if ABPM is administrated correctly and an autonomic protocol (including a diary) is followed which will be discussed in this review. A 24-h ABPM does not only allow the detection of OH, if it is present, but also the assessment of cardiovascular autonomic dysfunction during and after various daily stimuli, such as postprandial and alcohol dependent hypotension, as well as exercise and drug induced hypotension. Furthermore, information about the circadian rhythm of BP and heart rate (HR) can be obtained and establish whether or not a patient has a fall of BP at night (i.e., "dipper" vs. non-"dipper"). The information about nocturnal BP may also allow the investigation or detection of disorders such as sleep dysfunction, nocturnal movement disorders, and obstructive sleep apnea, which are common in PD. Additionally, a 24-h ABPM should be conducted to examine the effectiveness of OH therapy. This review will outline the methodology of 24 h ABPM in PD, summarize findings of such studies in PD, and briefly consider common daily stimuli that might affect 24 h ABPM.
Keywords: 24 h ambulatory blood pressure monitoring; Parkinson’s disease; autonomic protocol; circadian rhythm; non-dipping; non-invasive; orthostatic hypotension; supine hypertension.
Figures

References
-
- Alli C., Avanzini F., Bettelli G., Colombo F., Corso R., Di Tullio M., et al. (1992). Prevalence and variability of orthostatic hypotension in the elderly. Results of the ‘Italian study on blood pressure in the elderly (SPAA)’. The ‘Gruppo di Studio Sulla Pressione Arteriosa nell’Anziano’. Eur. Heart J. 13, 178–182 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical