

Outcomes after kidney transplantation of patients previously diagnosed with atrial fibrillation
- PMID: 23721555
- PMCID: PMC3670777
- DOI: 10.1111/ajt.12197
Outcomes after kidney transplantation of patients previously diagnosed with atrial fibrillation
Abstract
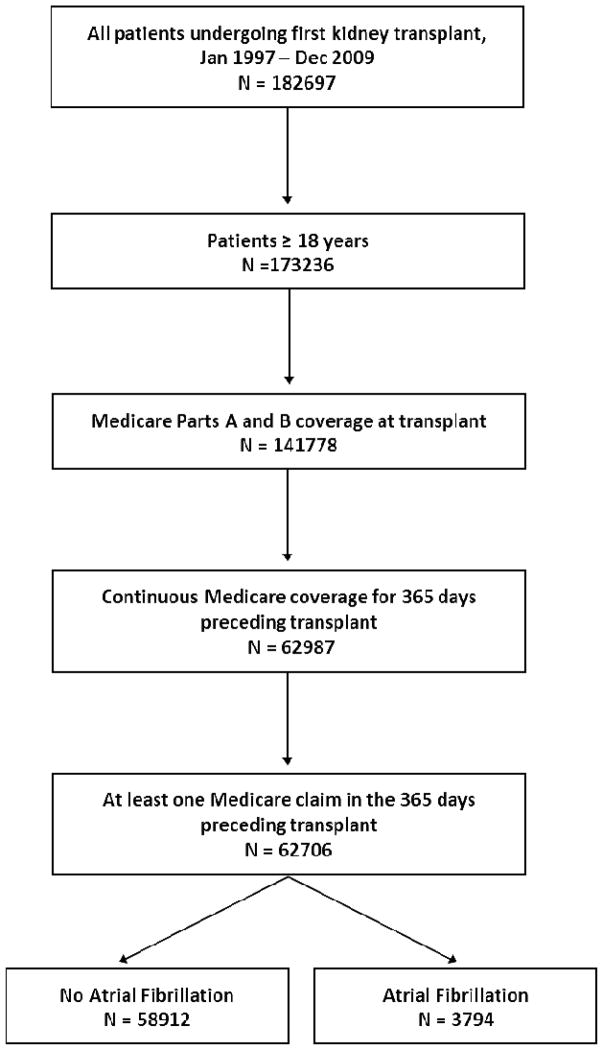
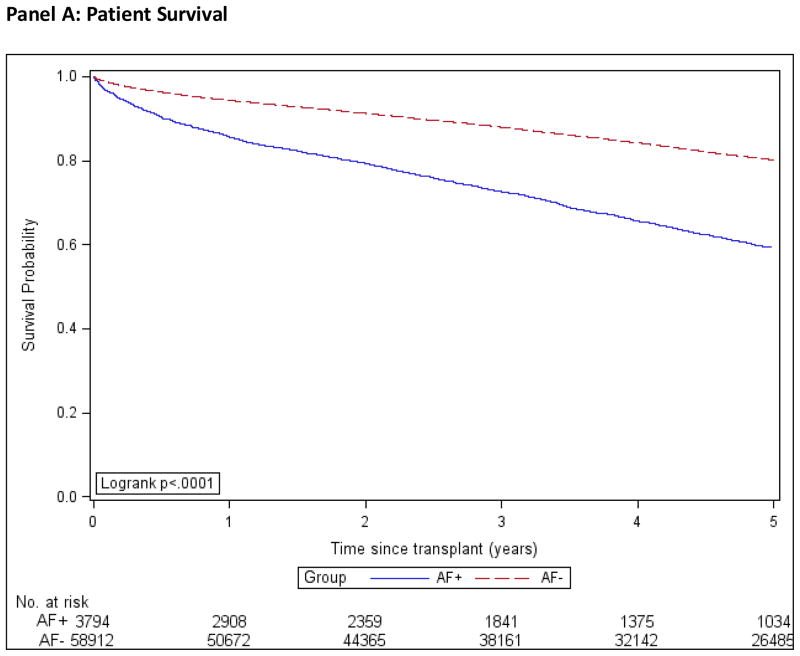
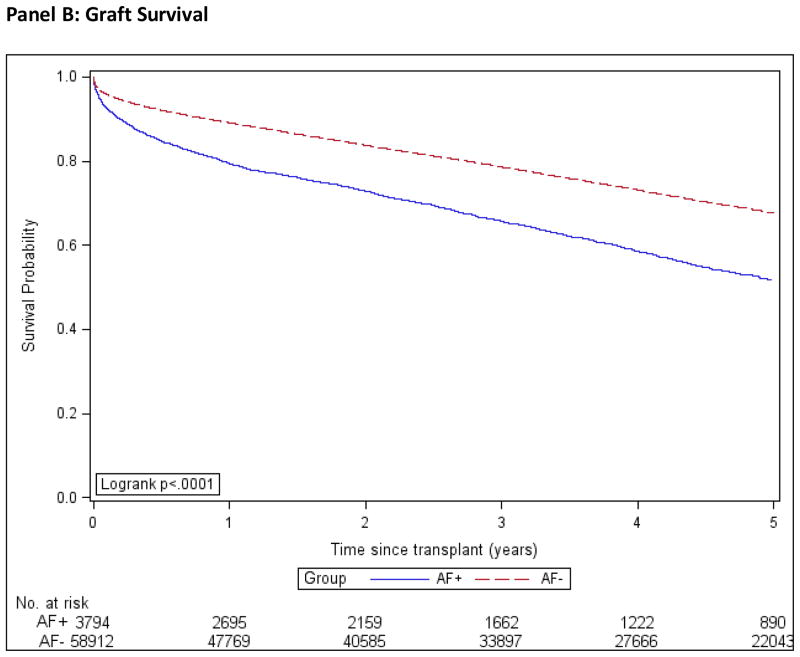
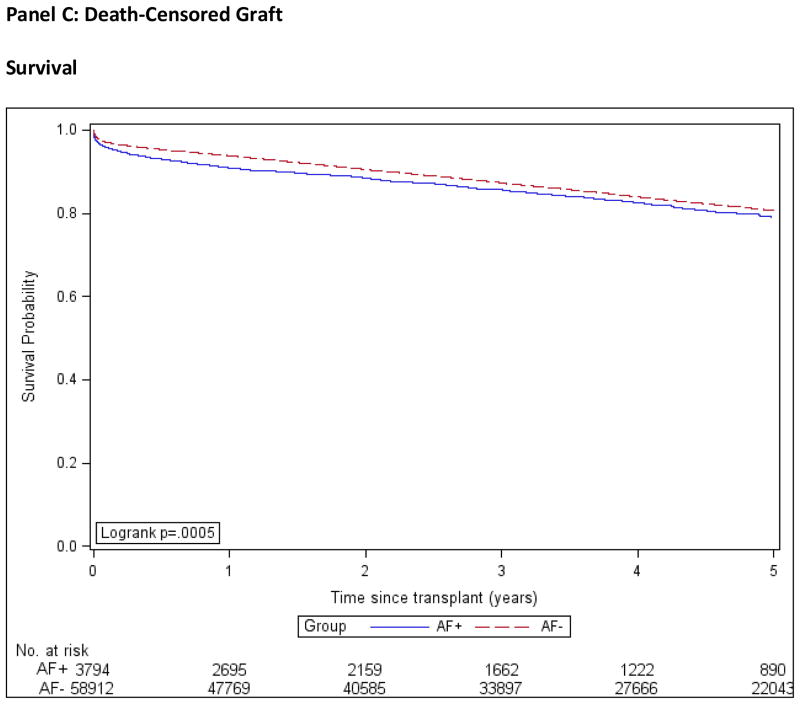
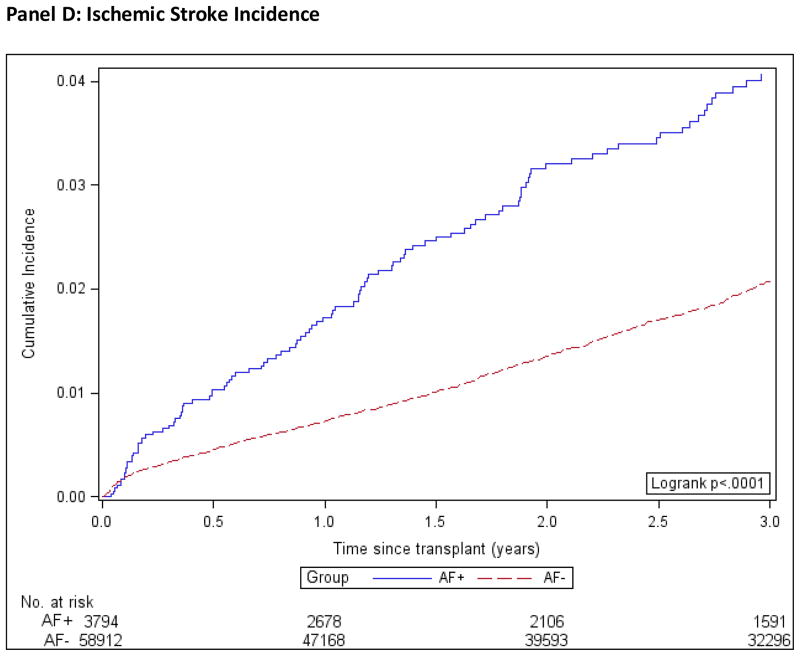
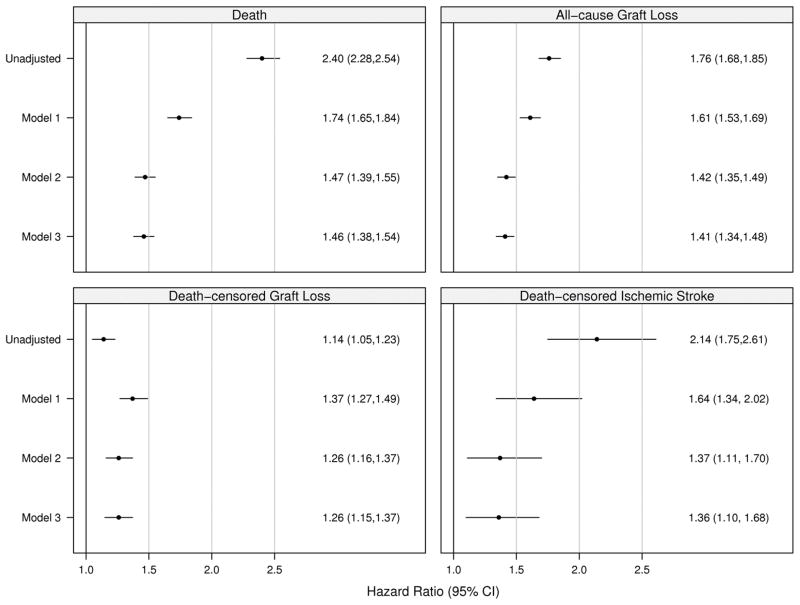
Little is known about the prevalence and outcomes of patients with atrial fibrillation/flutter (AF) who receive a kidney transplant. We identified all patients who had >1 year of uninterrupted Medicare A+B coverage before receiving their first kidney transplant (1997-2009). The presence of pretransplant AF was ascertained from diagnosis codes in Medicare physician claims. We studied the posttransplant outcomes of death, all-cause graft failure, death-censored graft failure and stroke using multivariable Cox regression. Of 62 706 eligible first kidney transplant recipients studied, 3794 (6.4%) were diagnosed with AF prior to kidney transplant. Over a mean follow up of 4.9 years, 40.6% of AF patients and 24.9% without AF died. All-cause and death-censored graft failure were 46.8% and 16.5%, respectively, in the AF group and 36.4% and 19.5%, respectively, in those without AF. Ischemic stroke occurred in 2.8% of patients with and 1.6% of patients without AF. In patients with AF, multivariable-adjusted hazard ratios (95% confidence intervals) for death, graft failure, death-censored graft failure and ischemic stroke were 1.46 (1.38-1.54), 1.41 (1.34-1.48), 1.26 (1.15-1.37) and 1.36 (1.10-1.68), respectively. Pre-existing AF is associated with poor posttransplant outcomes. Special attention should be paid to AF in pretransplant evaluation, counseling and risk stratification of kidney transplant candidates.
© Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119–125. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–988. - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946–952. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146(12):857–867. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
