

In vitro and in vivo imaging characteristics assessment of polymeric coils compared with standard platinum coils for the treatment of intracranial aneurysms
- PMID: 23721897
- PMCID: PMC7964839
- DOI: 10.3174/ajnr.A3589
In vitro and in vivo imaging characteristics assessment of polymeric coils compared with standard platinum coils for the treatment of intracranial aneurysms
Abstract
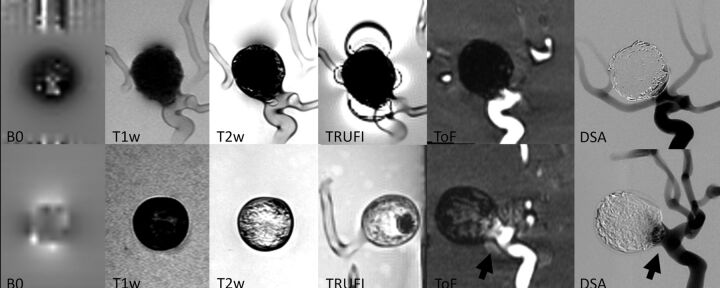
Background and purpose: Conventional platinum coils cause imaging artifacts that reduce imaging quality and therefore impair imaging interpretation on intraprocedural or noninvasive follow-up imaging. The purpose of this study was to evaluate imaging characteristics and artifact production of polymeric coils compared with standard platinum coils in vitro and in vivo.
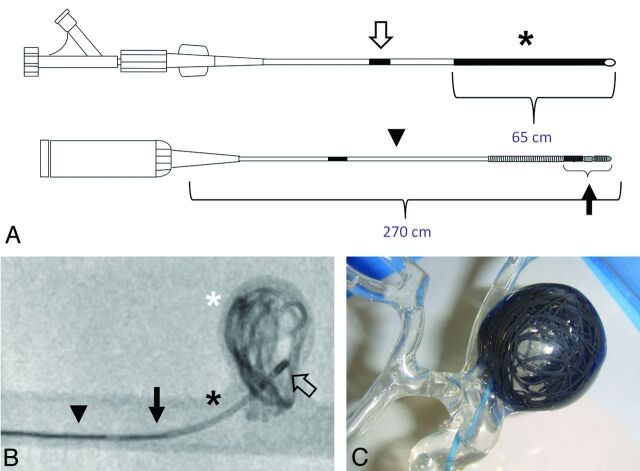
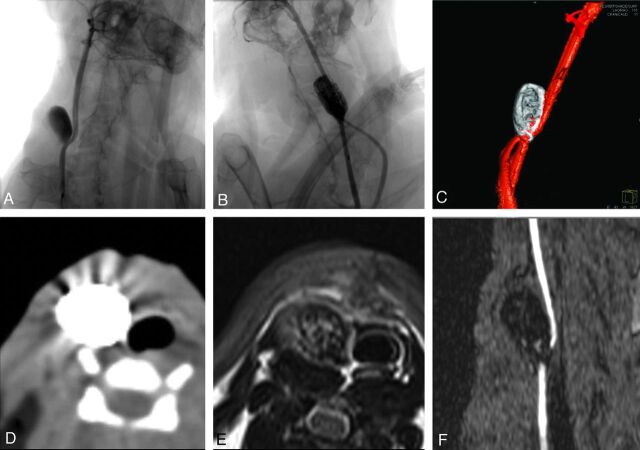
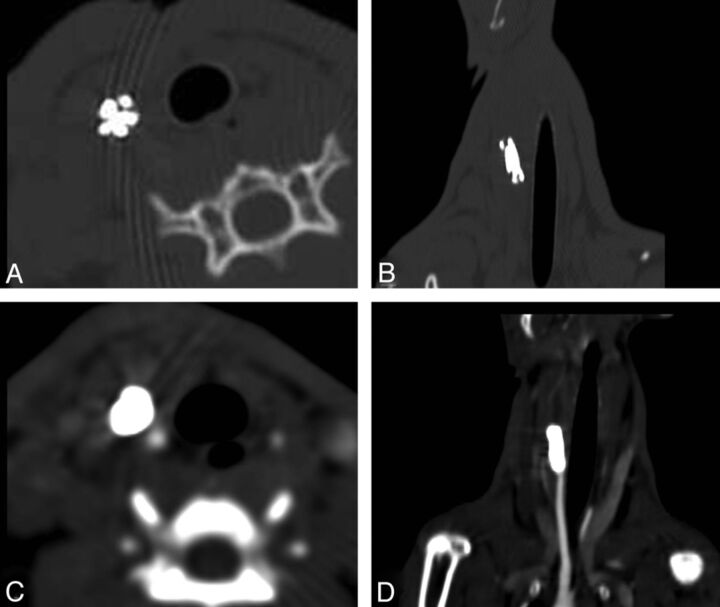
Materials and methods: Polymeric coils and standard platinum coils were evaluated in vitro with the use of 2 identical silicon aneurysm models coiled with a packing attenuation of 20% each. DSA, flat panel CT, CT, and MR imaging were performed. In vivo evaluation of imaging characteristics of polymeric coils was performed in experimentally created rabbit carotid bifurcation aneurysms. DSA, CT/CTA, and MR imaging were performed after endovascular treatment of the aneurysms. Images were evaluated regarding visibility of individual coils, coil mass, artifact production, and visibility of residual flow within the aneurysm.
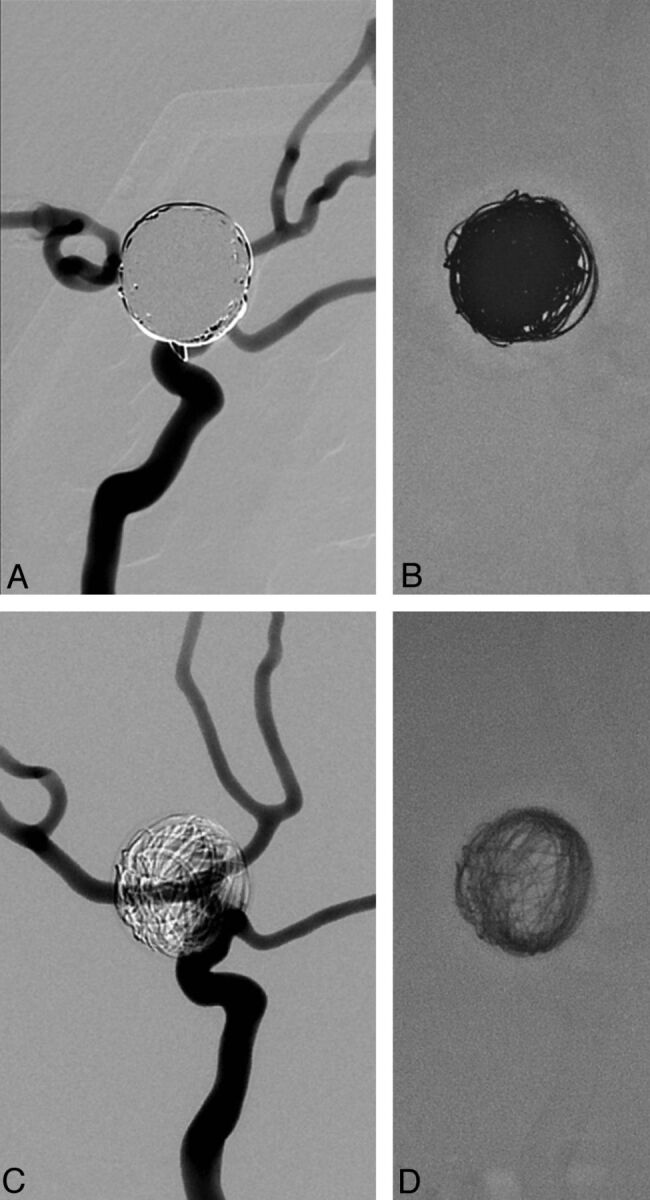
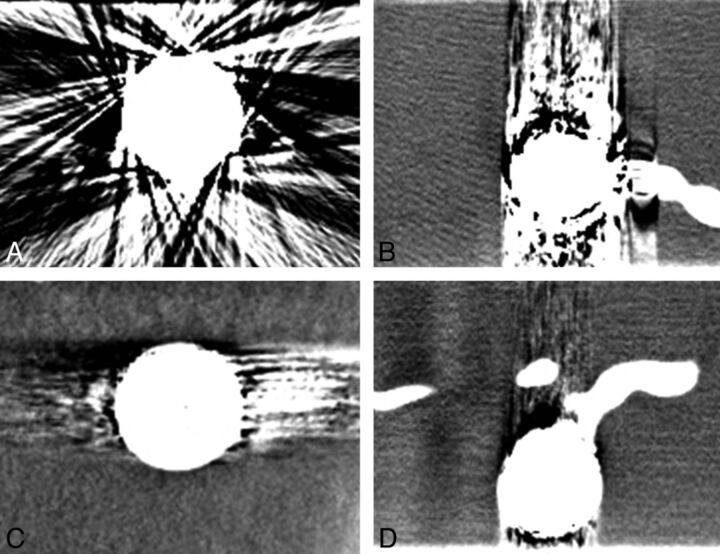
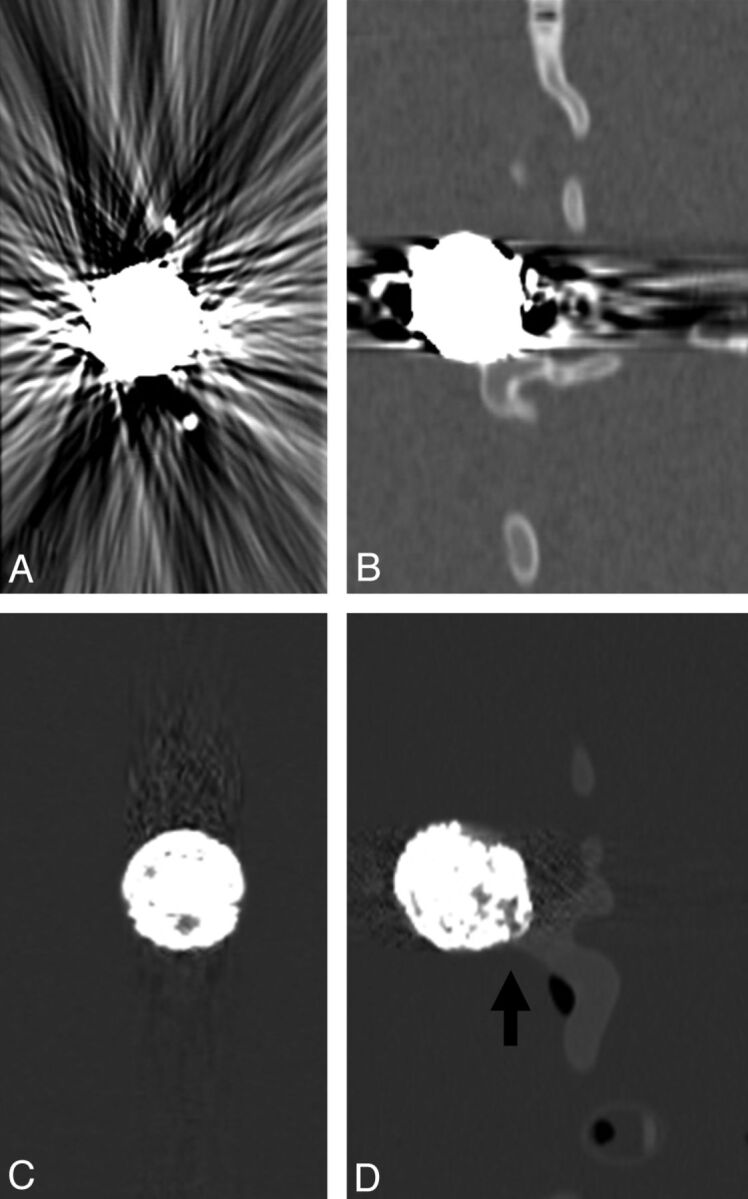
Results: Overall, in vitro and in vivo imaging showed relevantly reduced artifact production of polymeric coils in all imaging modalities compared with standard platinum coils. Image quality of CT and MR imaging was improved with the use of polymeric coils, which permitted enhanced depiction of individual coil loops and residual aneurysm lumen as well as the peri-aneurysmal area. Remarkably, CT images demonstrated considerably improved image quality with only minor artifacts compared with standard coils. On DSA, polymeric coils showed transparency and allowed visualization of superimposed vessel structures.
Conclusions: This initial experimental study showed improved imaging quality with the use of polymeric coils compared with standard platinum coils in all imaging modalities. This might be advantageous for improved intraprocedural imaging for the detection of complications and posttreatment noninvasive follow-up imaging.
Figures
References
-
- Molyneux AJ, Kerr RS, Yu LM, et al. . International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366:809–17 - PubMed
-
- Byrne JV, Sohn MJ, Molyneux AJ, et al. . Five-year experience in using coil embolization for ruptured intracranial aneurysms: outcomes and incidence of late rebleeding. J Neurosurg 1999;90:656–63 - PubMed
-
- Raymond J, Guilbert F, Weill A, et al. . Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 2003;34:1398–403 - PubMed
-
- Kang HS, Han MH, Kwon BJ, et al. . Repeat endovascular treatment in post-embolization recurrent intracranial aneurysms. Neurosurgery 2006;58:60–70 - PubMed
-
- Campi A, Ramzi N, Molyneux AJ, et al. . Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2007;38:1538–44 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical