

Review
doi: 10.1102/1470-7330.2013.0024.
Imaging appearance of sarcomas of the prostate
Affiliations
- PMID: 23722584
- PMCID: PMC3667567
- DOI: 10.1102/1470-7330.2013.0024
Item in Clipboard
Review
Imaging appearance of sarcomas of the prostate
Cancer Imaging.
.
Abstract
Sarcomas of the prostate are rare tumours. Their clinicopathologic features are well described, however, the imaging features of these tumours have rarely been documented. The purpose of this article is to illustrate the imaging findings of prostate sarcomas, with an emphasis on their appearance on magnetic resonance imaging and to identify features that may help to differentiate them from the commoner prostate adenocarcinomas.
Figures

A 17-year-old male (a, b) and 15-year old male (c) both with a prostatic alveolar rhabdomyosarcoma. (a) Sagittal T2-weighted and (b) coronal T2-weighted MR images show the prostate tumour as an irregular, ill-defined soft tissue mass, which is predominantly of intermediate T2 signal intensity. It extends beyond the prostate, breaching the urogenital diaphragm, extending into the penile bulb (black arrow) and invades the anterior wall of the rectum (white arrow). (c) Axial T2-weighted MR images. The tumour demonstrates the aggressive infiltrative features of alveolar rhabdomyosaromas, invading the seminal vesicles, vas deferens (black open arrow), bladder and extending up to the mesorectal fascia posteriorly. There are enlarged left pelvic side wall nodes (white asterisk). Ascites is also noted (black asterisk).
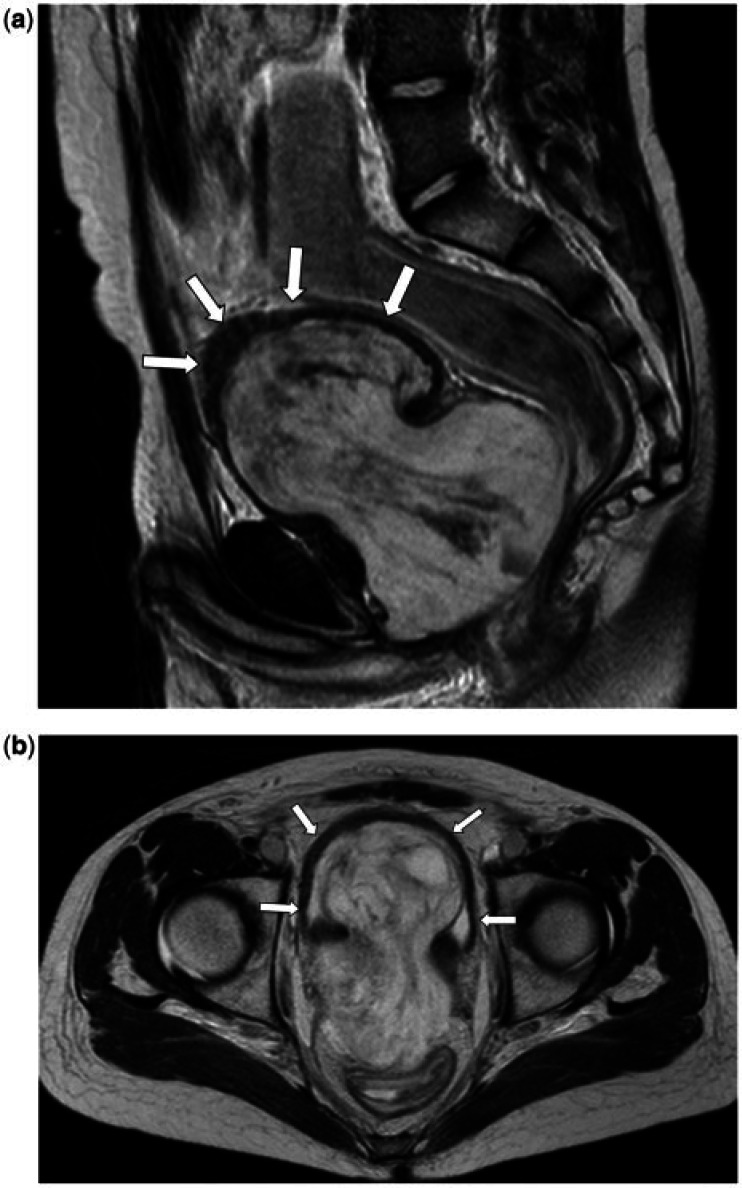
A 15-year-old male with a prostatic embryonal rhabdomyosarcoma. (a) Sagittal T2-weighted and (b) axial T2-weighted images show the tumour as a well-defined lobulated mass that replaces and extends beyond the prostate, exerting a mass effect anteriorly on the bladder (arrows) and on the lower rectum posteriorly. The mass consists of a T2 hyperintense stroma containing sheets of intermediate-low signal tissue.
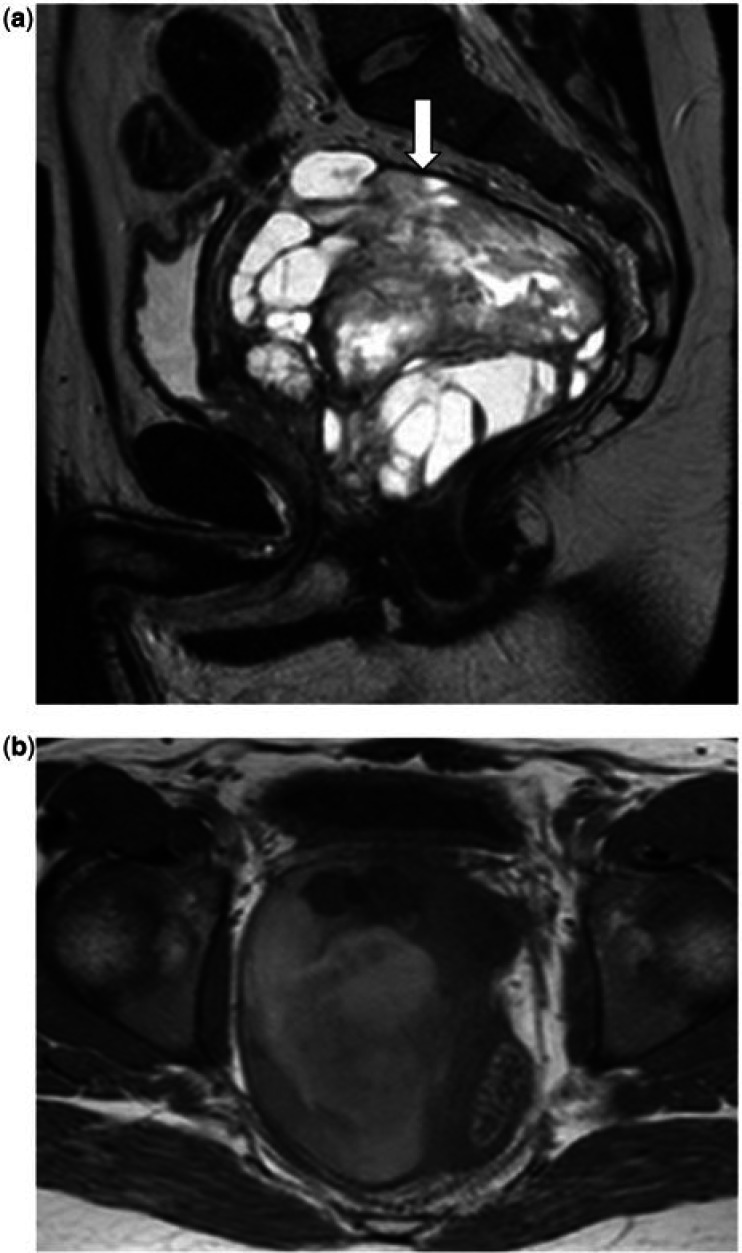
A 33-year-old man with a MPNST of the prostate. (a) Sagittal T2-weighted MR image shows the tumour as a very heterogeneous mass, with areas of high, intermediate and low T2 signal seen within it, and areas of necrosis/cystic change. The mass is well defined with a T2 low signal intensity pseudocapsule seen along its superior and posterior border (white arrow). (b) Axial T1-weighted MR image shows that the mass is heterogeneous; the tumour is of relatively low T1 signal but contains areas of T1 high signal intensity in keeping with haemorrhage.
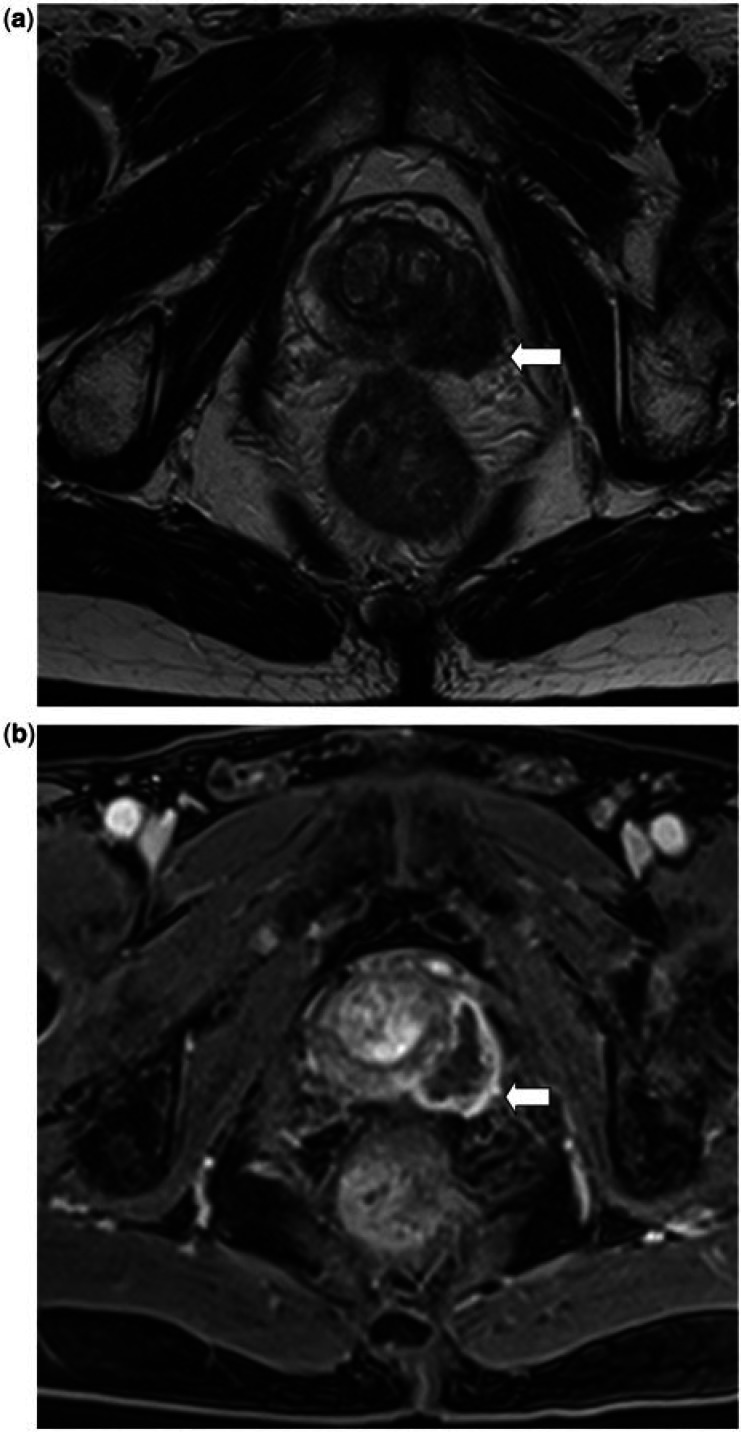
A 63-year-old man with a prostatic leiomyosarcoma. (a) Axial T2-weighted MR image shows a slightly ill-defined lesion arising from the peripheral zone of the prostate, which is predominantly of homogeneous low T2 signal intensity and shows extension into the transition zone and extracapsular extension. (b) Axial T1-weighted fat-suppressed postcontrast MR image demonstrates avid peripheral enhancement of the tumour with central necrosis.
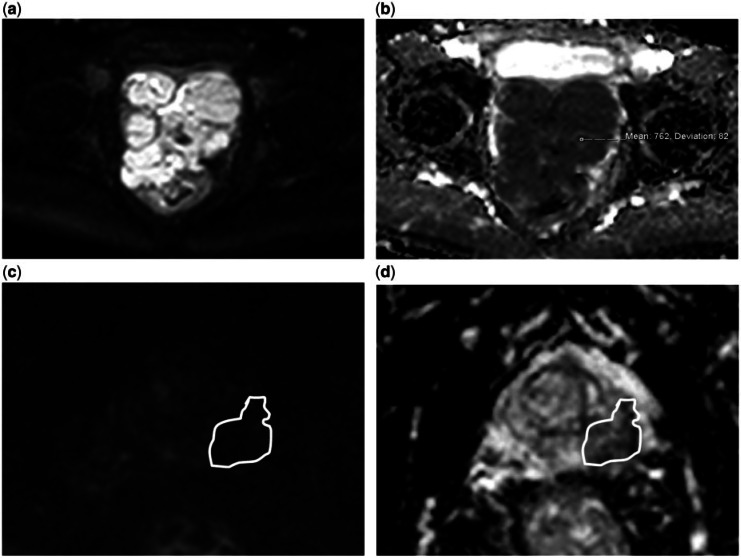
A 54-year-old man (a, b) and a 62-year-old man (c, d), both with a prostatic leiomyosarcoma. The images show the different diffusion appearances between the 2 cases. (a) DW image with a b value of 1000 s/mm2 and (b) ADC map shows that the tumour demonstrates impeded diffusion and has a mean ADC value of 0.76 × 10–3 mm2/s. (c) DW image with a b value of 1000 s/mm2 and (d) ADC map shows that this tumour does not demonstrate impeded diffusion and has a mean ADC value of 0.51 × 10–3 mm2/s but is also of low signal on the b1000 image.
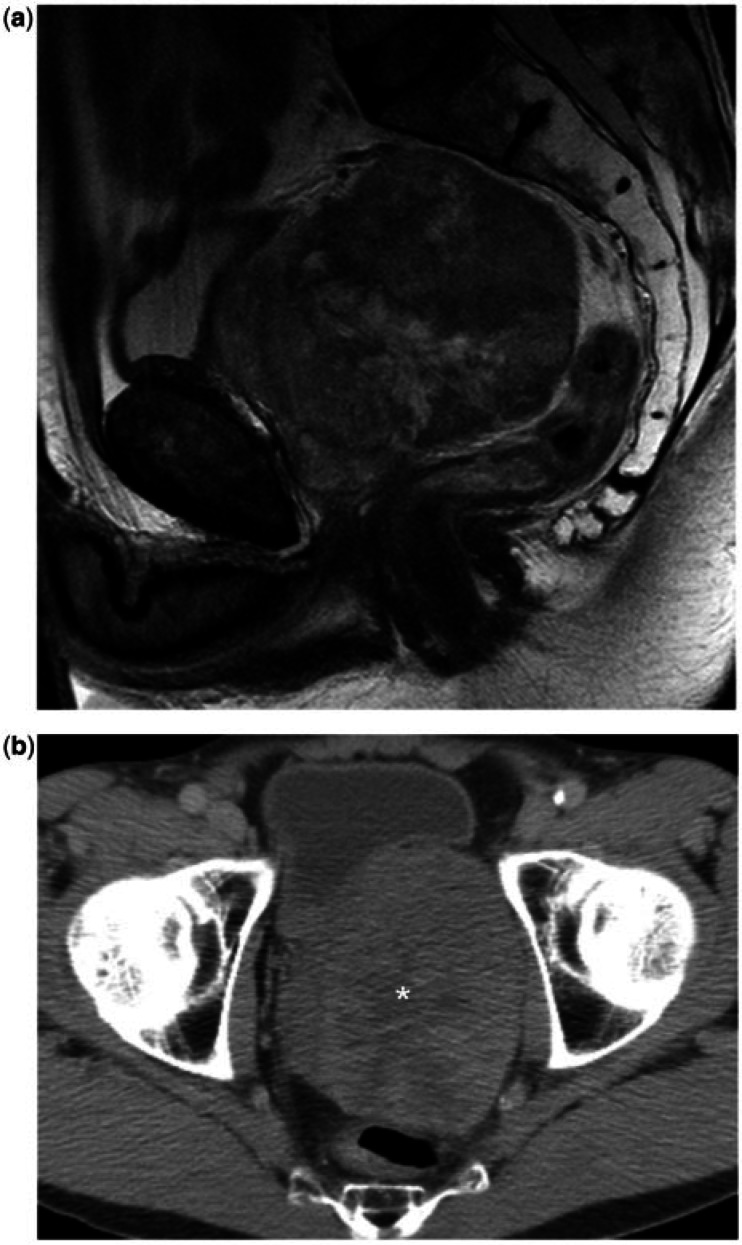
A 54-year-old man with a prostatic leiomyosarcoma. (A) Sagittal T2-weighted MR image shows the tumour as a large, well-defined, rounded mass arising from the superior aspect of the prostate, with heterogeneous T2 signal intensity. (b) Axial CT image shows the lesion as a heterogeneous mass, containing areas of necrosis/cystic change (asterisk).
References
-
- Eble JN, Sauter G, Epstein JI, Sesterhann IA. World Health Organization classification of tumours. Pathology and genetics of tumours of the urinary system and male genital organs. Lyon: IARC Press; 2004. pp. p. 1–354.
-
- Tetu B, Srigley JR, Bostwick DG. Soft tissue tumours. In: Bostwick DG, editor. Pathology of the prostate. New York: Churchill Livingstone; 1990. p. p. 117.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical