

Can tidal breathing with deep inspirations of intact airways create sustained bronchoprotection or bronchodilation?
- PMID: 23722710
- PMCID: PMC3742943
- DOI: 10.1152/japplphysiol.00009.2013
Can tidal breathing with deep inspirations of intact airways create sustained bronchoprotection or bronchodilation?
Abstract
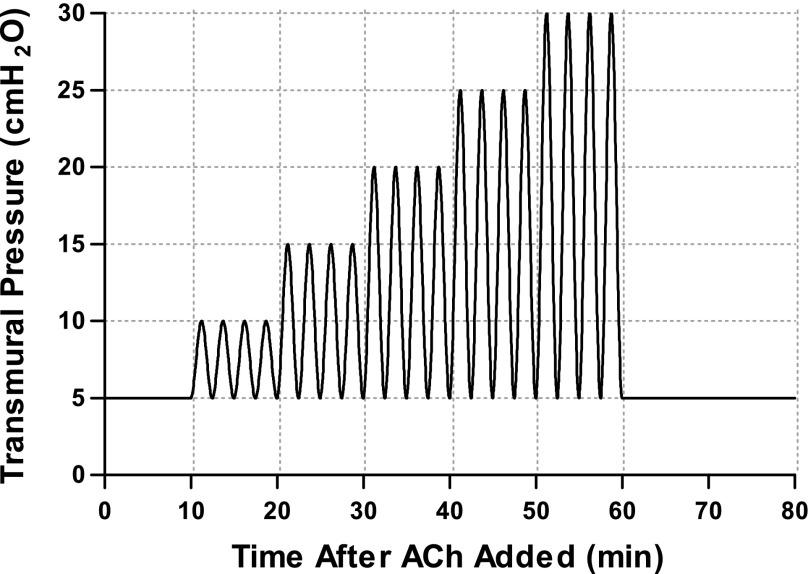
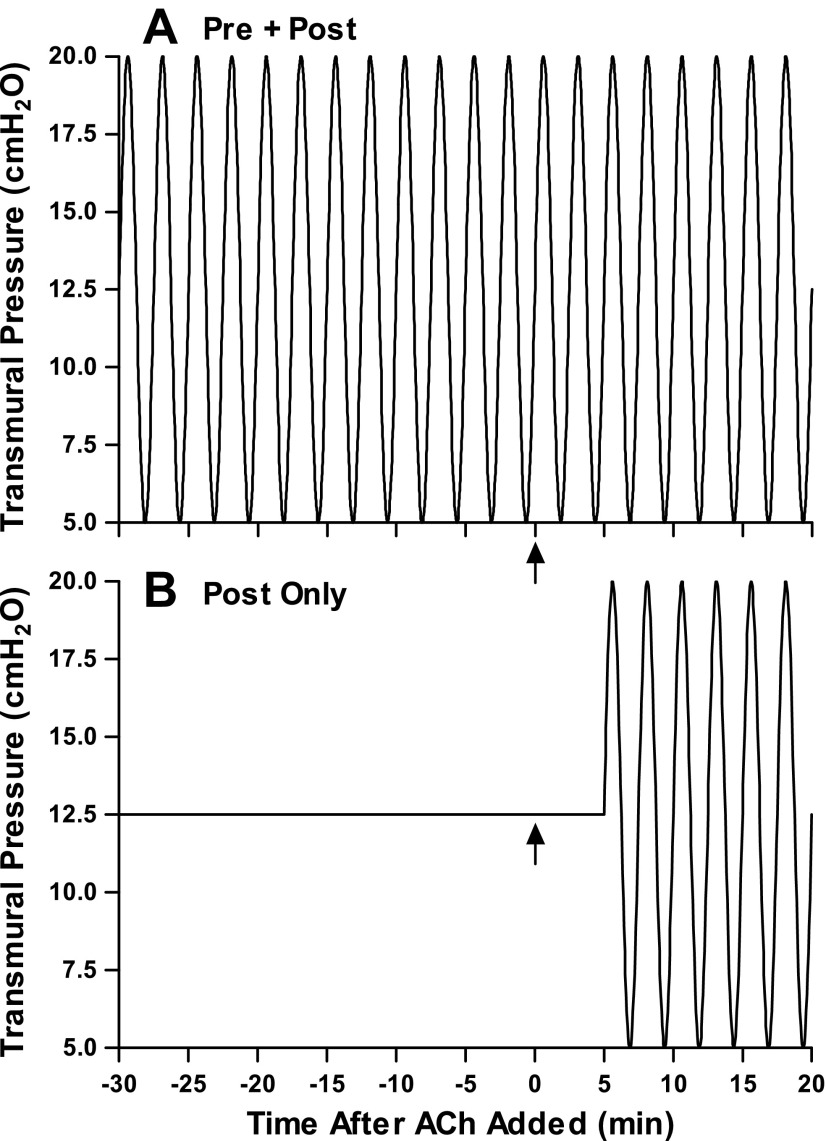
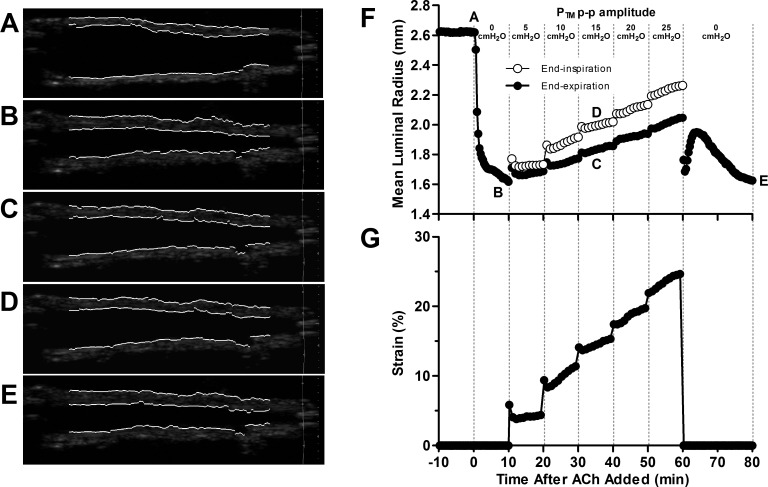
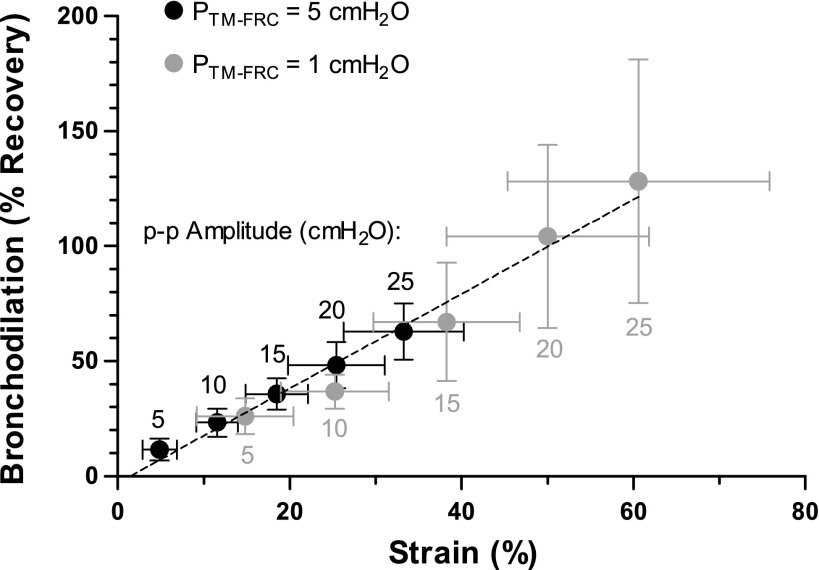
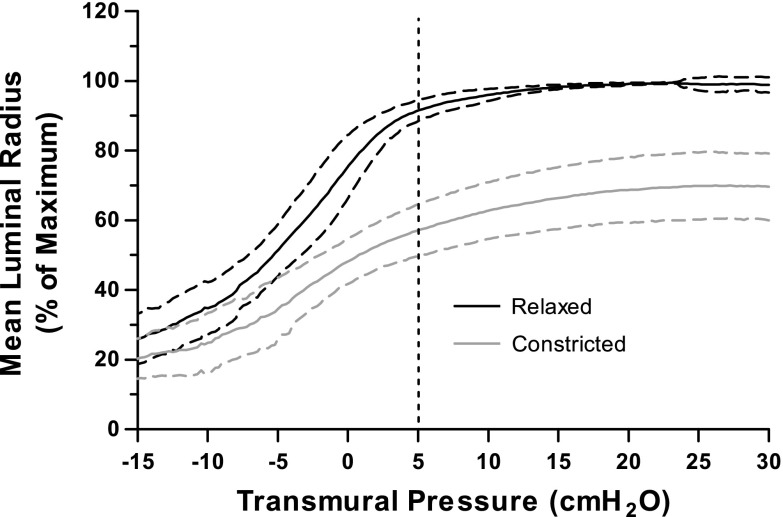
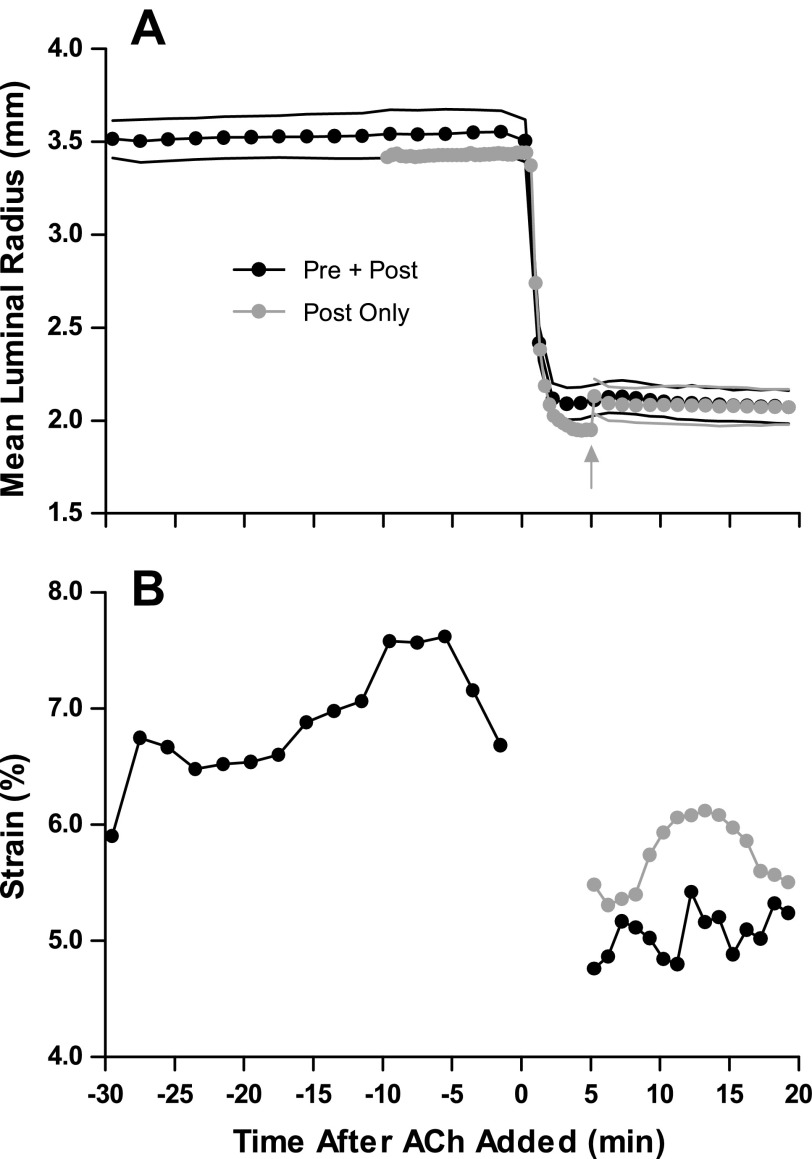
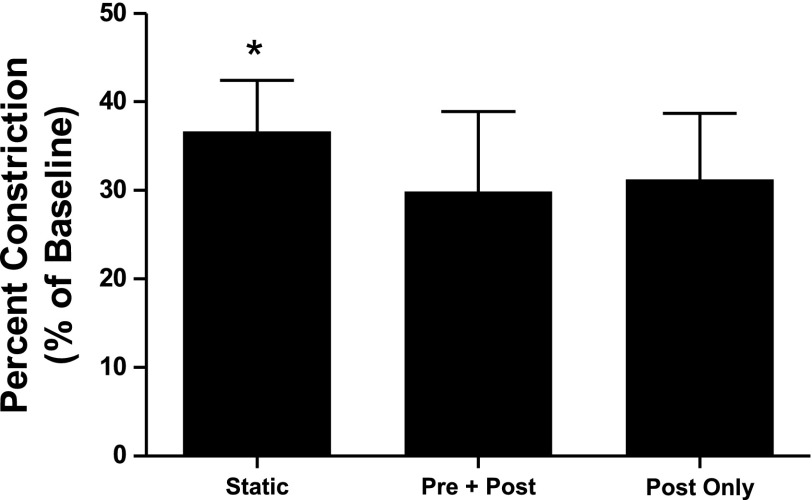
Fluctuating forces imposed on the airway smooth muscle due to breathing are believed to regulate hyperresponsiveness in vivo. However, recent animal and human isolated airway studies have shown that typical breathing-sized transmural pressure (Ptm) oscillations around a fixed mean are ineffective at mitigating airway constriction. To help understand this discrepancy, we hypothesized that Ptm oscillations capable of producing the same degree of bronchodilation as observed in airway smooth muscle strip studies requires imposition of strains larger than those expected to occur in vivo. First, we applied increasingly larger amplitude Ptm oscillations to a statically constricted airway from a Ptm simulating normal functional residual capacity of 5 cmH2O. Tidal-like oscillations (5-10 cmH2O) imposed 4.9 ± 2.0% strain and resulted in 11.6 ± 4.8% recovery, while Ptm oscillations simulating a deep inspiration at every breath (5-30 cmH2O) achieved 62.9 ± 12.1% recovery. These same Ptm oscillations were then applied starting from a Ptm = 1 cmH2O, resulting in approximately double the strain for each oscillation amplitude. When extreme strains were imposed, we observed full recovery. On combining the two data sets, we found a linear relationship between strain and resultant recovery. Finally, we compared the impact of Ptm oscillations before and after constriction to Ptm oscillations applied only after constriction and found that both loading conditions had a similar effect on narrowing. We conclude that, while sufficiently large strains applied to the airway wall are capable of producing substantial bronchodilation, the Ptm oscillations necessary to achieve those strains are not expected to occur in vivo.
Keywords: airway smooth muscle; asthma; bronchodilation; bronchoprotection; intact airways.
Figures
References
-
- Ansell TK, Noble PB, Mitchell HW, West AR, Fernandes LB, McFawn PK. Effects of simulated tidal and deep breathing on immature airway contraction to acetylcholine and nerve stimulation. Respirology 14: 991–998, 2009 - PubMed
-
- Bates JHT, Maksym GN. Mechanical determinants of airways hyperresponsiveness. Crit Rev Biomed Eng 39: 281–296, 2011 - PubMed
-
- Bendixen HH, Smith GM, Mead J. Pattern of ventilation in young adults. J Appl Physiol 19: 195–198, 1964 - PubMed
-
- Berry EM, Edmonds JF, Wyllie H. Release of prostaglandin E2 and unidentified factors from ventilated lungs. Br J Surg 58: 189–192, 1971 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources