

Comparative efficacy of seven psychotherapeutic interventions for patients with depression: a network meta-analysis
- PMID: 23723742
- PMCID: PMC3665892
- DOI: 10.1371/journal.pmed.1001454
Comparative efficacy of seven psychotherapeutic interventions for patients with depression: a network meta-analysis
Abstract
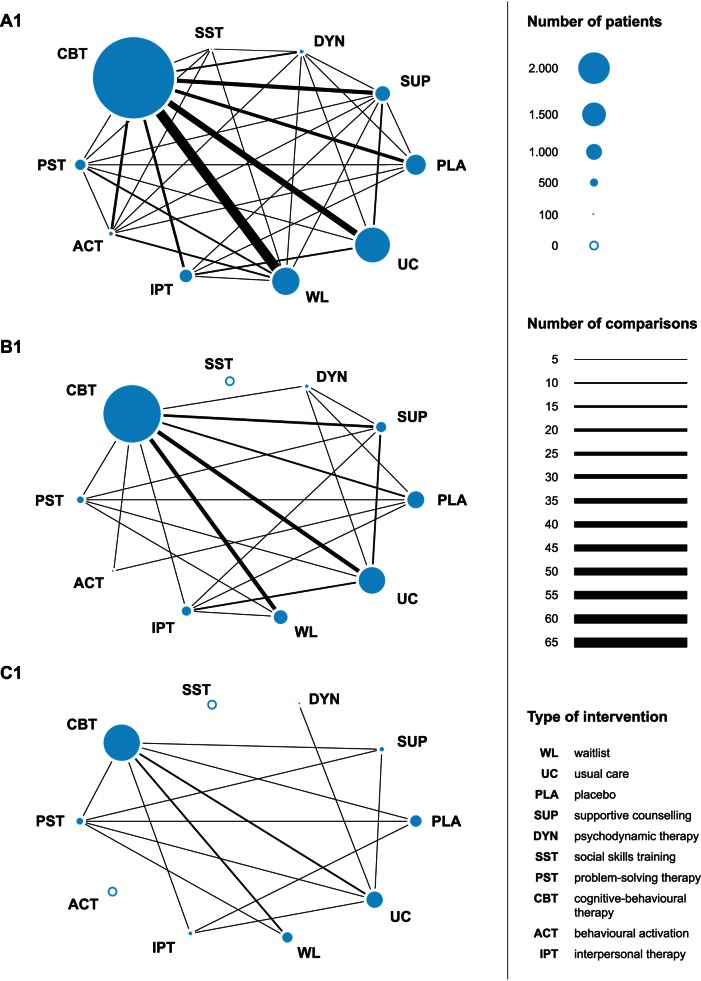
Background: Previous meta-analyses comparing the efficacy of psychotherapeutic interventions for depression were clouded by a limited number of within-study treatment comparisons. This study used network meta-analysis, a novel methodological approach that integrates direct and indirect evidence from randomised controlled studies, to re-examine the comparative efficacy of seven psychotherapeutic interventions for adult depression.
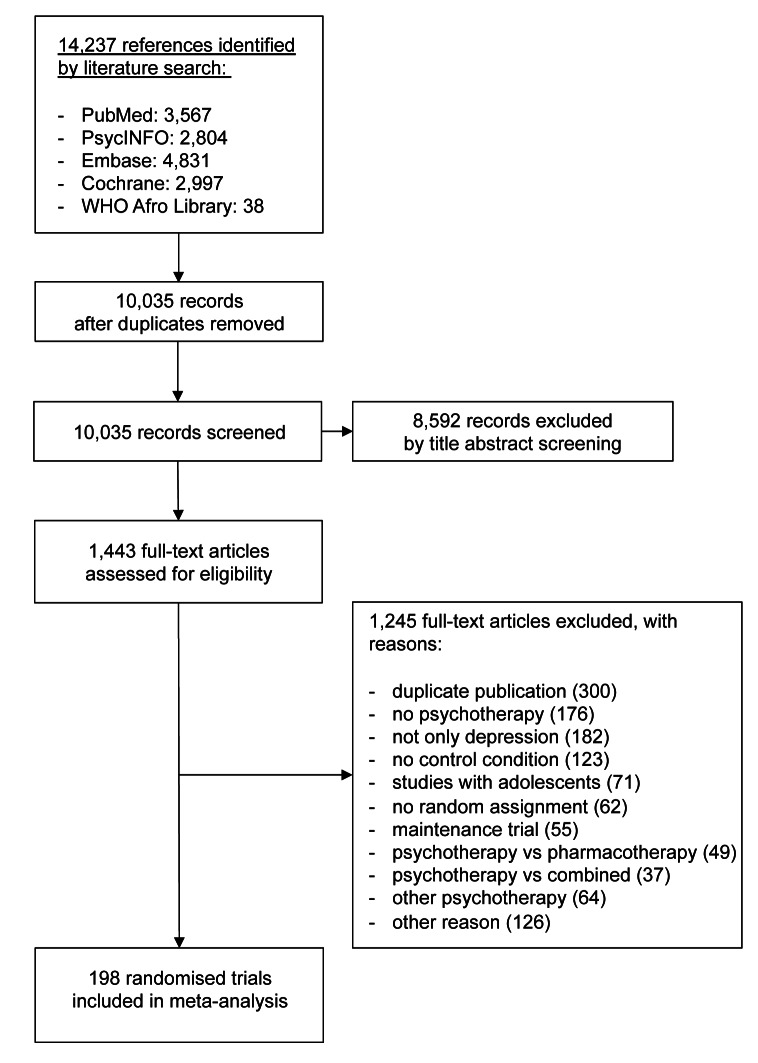
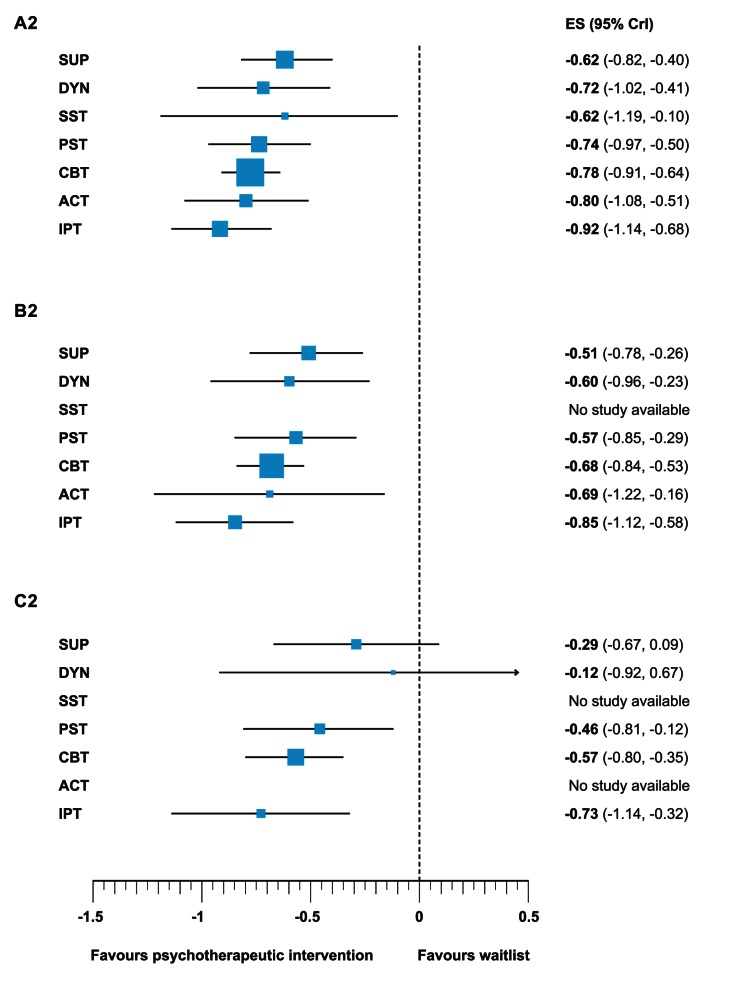
Methods and findings: We conducted systematic literature searches in PubMed, PsycINFO, and Embase up to November 2012, and identified additional studies through earlier meta-analyses and the references of included studies. We identified 198 studies, including 15,118 adult patients with depression, and coded moderator variables. Each of the seven psychotherapeutic interventions was superior to a waitlist control condition with moderate to large effects (range d = -0.62 to d = -0.92). Relative effects of different psychotherapeutic interventions on depressive symptoms were absent to small (range d = 0.01 to d = -0.30). Interpersonal therapy was significantly more effective than supportive therapy (d = -0.30, 95% credibility interval [CrI] [-0.54 to -0.05]). Moderator analysis showed that patient characteristics had no influence on treatment effects, but identified aspects of study quality and sample size as effect modifiers. Smaller effects were found in studies of at least moderate (Δd = 0.29 [-0.01 to 0.58]; p = 0.063) and large size (Δd = 0.33 [0.08 to 0.61]; p = 0.012) and those that had adequate outcome assessment (Δd = 0.38 [-0.06 to 0.87]; p = 0.100). Stepwise restriction of analyses by sample size showed robust effects for cognitive-behavioural therapy, interpersonal therapy, and problem-solving therapy (all d>0.46) compared to waitlist. Empirical evidence from large studies was unavailable or limited for other psychotherapeutic interventions.
Conclusions: Overall our results are consistent with the notion that different psychotherapeutic interventions for depression have comparable benefits. However, the robustness of the evidence varies considerably between different psychotherapeutic treatments.
Conflict of interest statement
PJ is an unpaid member of steering group or executive committee of trials funded by Abbott Vascular, Biosensors, Medtronic and St. Jude Medical. CTU Bern, which is part of the University of Bern, has a staff policy of not accepting individual honoraria or consultancy fees. However, CTU Bern is involved in design, conduct, or analysis of clinical studies funded by Abbott Vascular, Ablynx, Amgen, AstraZeneca, Biosensors, Biotronic, Boehrhinger Ingelheim, Eisai, Eli Lilly, Exelixis, Geron, Gilead Sciences, Nestlé, Novartis, Novo Nordisc, Padma, Roche, Schering-Plough, St. Jude Medical, and Swiss Cardio Technologies. The other authors declare that no competing interests exist.
Figures
Comment in
-
Review: different psychotherapies have comparable effects on adult depression.Evid Based Ment Health. 2013 Nov;16(4):122. doi: 10.1136/eb-2013-101522. Epub 2013 Oct 3. Evid Based Ment Health. 2013. PMID: 24091618 No abstract available.
References
-
- Blazer DG, Kessler RC, McGonagle KA, Swartz MS (1994) The prevalence and distribution of major depression in a national community sample: the National Comorbidity Survey. Am J Psychiatry 151: 979–986. - PubMed
-
- Jacobi F, Wittchen HU, Holting C, Hofler M, Pfister H, et al. (2004) Prevalence, co-morbidity and correlates of mental disorders in the general population: Results from the German Health Interview and Examination Survey (GHS). Psychol Med 34: 597–611. - PubMed
-
- Wittchen HU, Jacobi F (2005) Size and burden of mental disorders in Europe–a critical review and appraisal of 27 studies. Eur Neuropsychopharmacol 15: 357–376. - PubMed
-
- Cuijpers P, Andersson G, Donker T, van Straten A (2011) Psychological treatment of depression: results of a series of meta-analyses. Nordic J Psychiatry 65: 354–364. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
