

A pilot study of an mHealth application for healthcare workers: poor uptake despite high reported acceptability at a rural South African community-based MDR-TB treatment program
- PMID: 23724075
- PMCID: PMC3665589
- DOI: 10.1371/journal.pone.0064662
A pilot study of an mHealth application for healthcare workers: poor uptake despite high reported acceptability at a rural South African community-based MDR-TB treatment program
Abstract
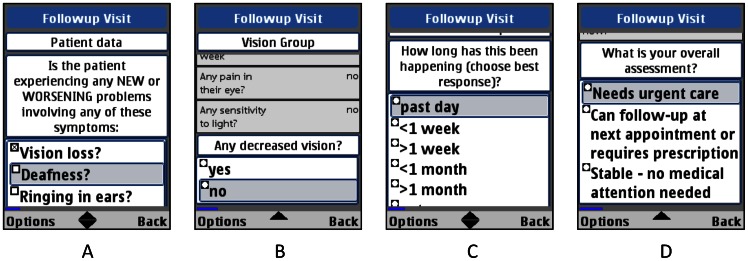
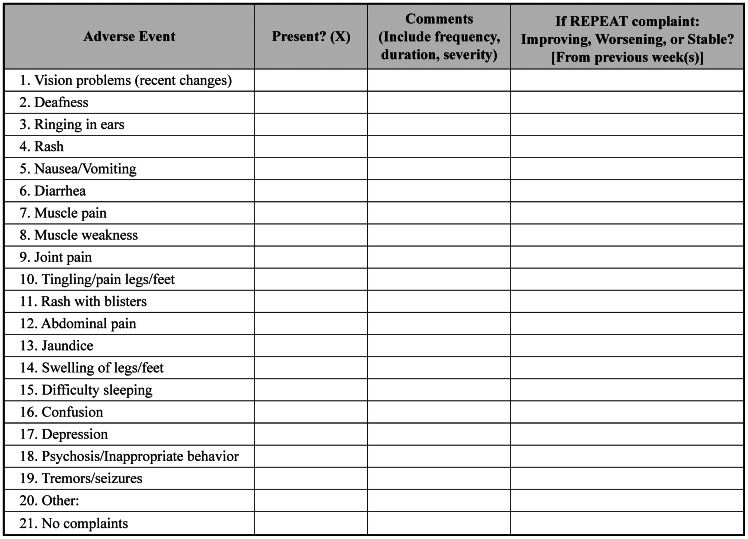
Introduction: As the South African province of KwaZulu-Natal addresses a growing multidrug-resistant tuberculosis (MDR-TB) epidemic by shifting care and treatment from trained specialty centers to community hospitals, delivering and monitoring MDR-TB therapy has presented new challenges. In particular, tracking and reporting adverse clinical events have been difficult for mobile healthcare workers (HCWs), trained health professionals who travel daily to patient homes to administer and monitor therapy. We designed and piloted a mobile phone application (Mobilize) for mobile HCWs that electronically standardized the recording and tracking of MDR-TB patients on low-cost, functional phones.
Objective: We assess the acceptability and feasibility of using Mobilize to record and submit adverse events forms weekly during the intensive phase of MDR-TB therapy and evaluate mobile HCW perceptions throughout the pilot period.
Methods: All five mobile HCWs at one site were trained and provided with phones. Utilizing a mixed-methods evaluation, mobile HCWs' usage patterns were tracked electronically for seven months and analyzed. Qualitative focus groups and questionnaires were designed to understand the impact of mobile phone technology on the work environment.
Results: Mobile HCWs submitted nine of 33 (27%) expected adverse events forms, conflicting with qualitative results in which mobile HCWs stated that Mobilize improved adverse events communication, helped their daily workflow, and could be successfully expanded to other health interventions. When presented with the conflict between their expressed views and actual practice, mobile HCWs cited forgetfulness and believed patients should take more responsibility for their own care.
Discussion: This pilot experience demonstrated poor uptake by HCWs despite positive responses to using mHealth. Though our results should be interpreted cautiously because of the small number of mobile HCWs and MDR-TB patients in this study, we recommend carefully exploring the motivations of HCWs and technologic enhancements prior to scaling new mHealth initiatives in resource poor settings.
Conflict of interest statement
Figures
References
-
- World Health Organization (2012) Global tuberculosis control 2012. Geneva: World Health Organization.
-
- Gandhi NR, Shah NS, Andrews JR, Vella V, Moll AP, et al. (2010) HIV coinfection in multidrug- and extensively drug-resistant tuberculosis results in high early mortality. Am J Respir Crit Care Med 181: 80–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
