

Tricuspid annular geometry: a three-dimensional transesophageal echocardiographic study
- PMID: 23725682
- PMCID: PMC3821008
- DOI: 10.1053/j.jvca.2012.12.014
Tricuspid annular geometry: a three-dimensional transesophageal echocardiographic study
Abstract
Objective: To demonstrate the clinical feasibility of accurately measuring tricuspid annular area by 3-dimensional (3D) transesophageal echocardiography (TEE) and to assess the geometric differences based on the presence of tricuspid regurgitation (TR). Also, the shape of the tricuspid annulus was compared with previous descriptions in the literature.
Design: Prospective.
Setting: Tertiary care university hospital.
Interventions: Three-dimensional TEE.
Participants: Patients undergoing cardiac surgery.
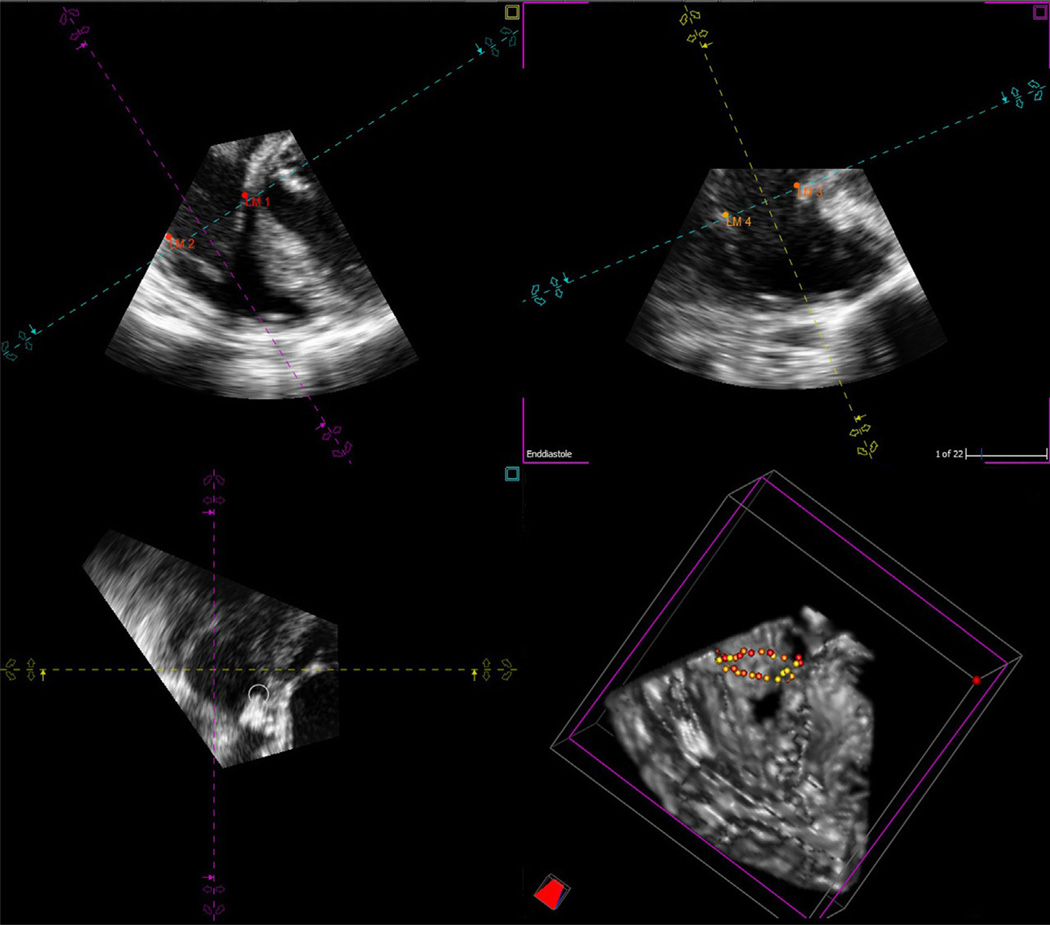
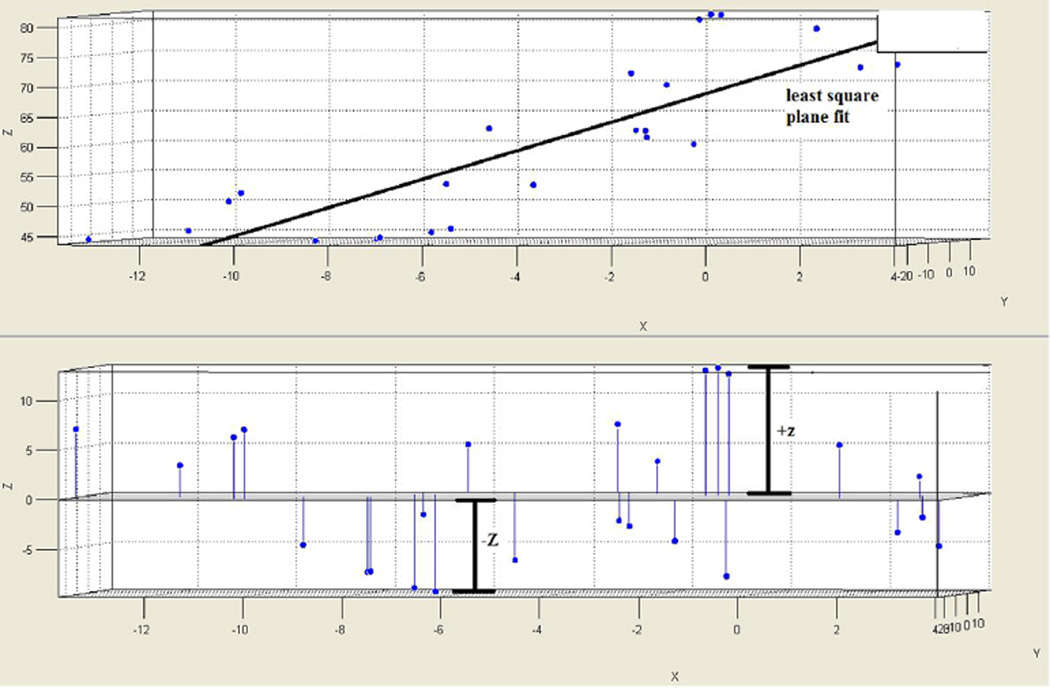
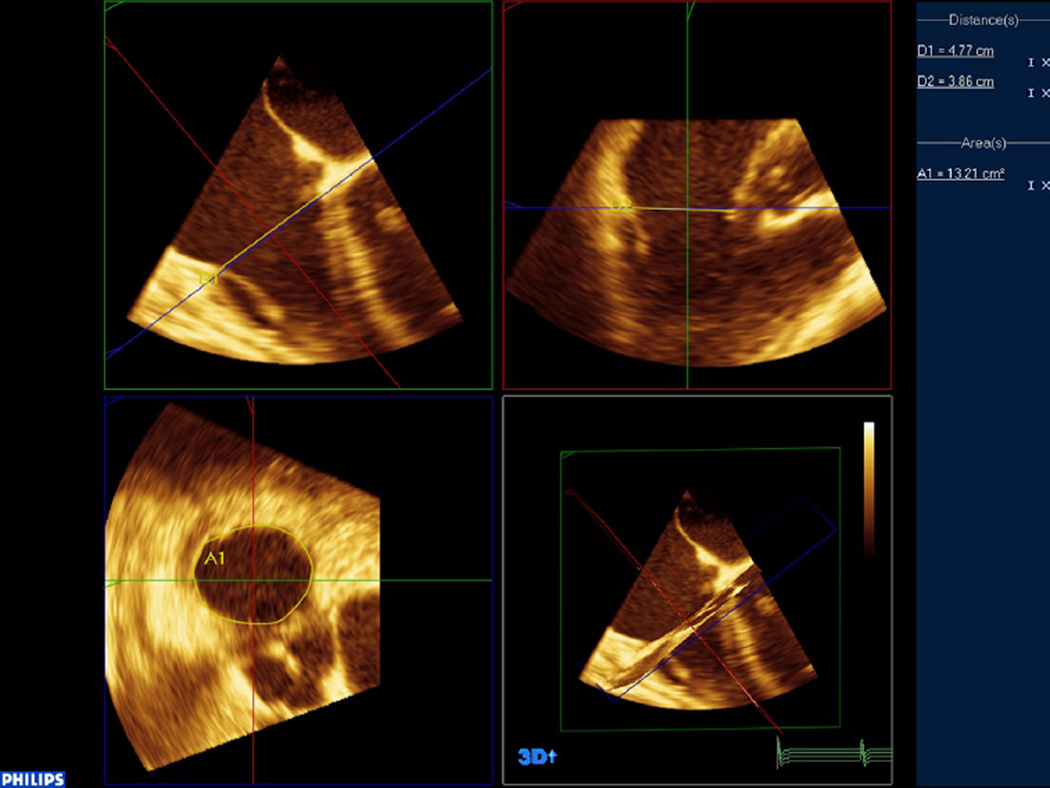
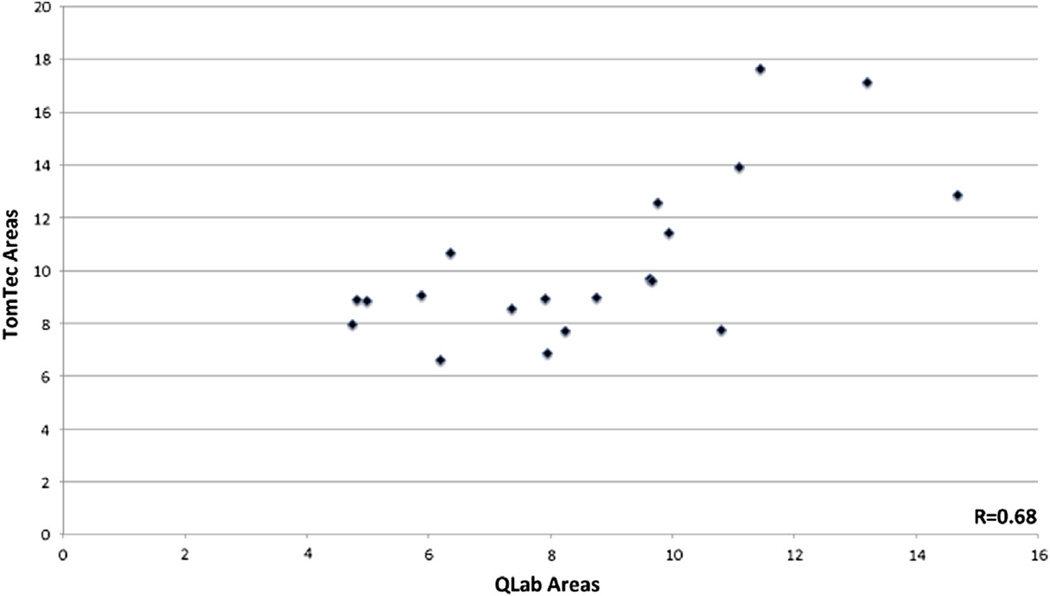
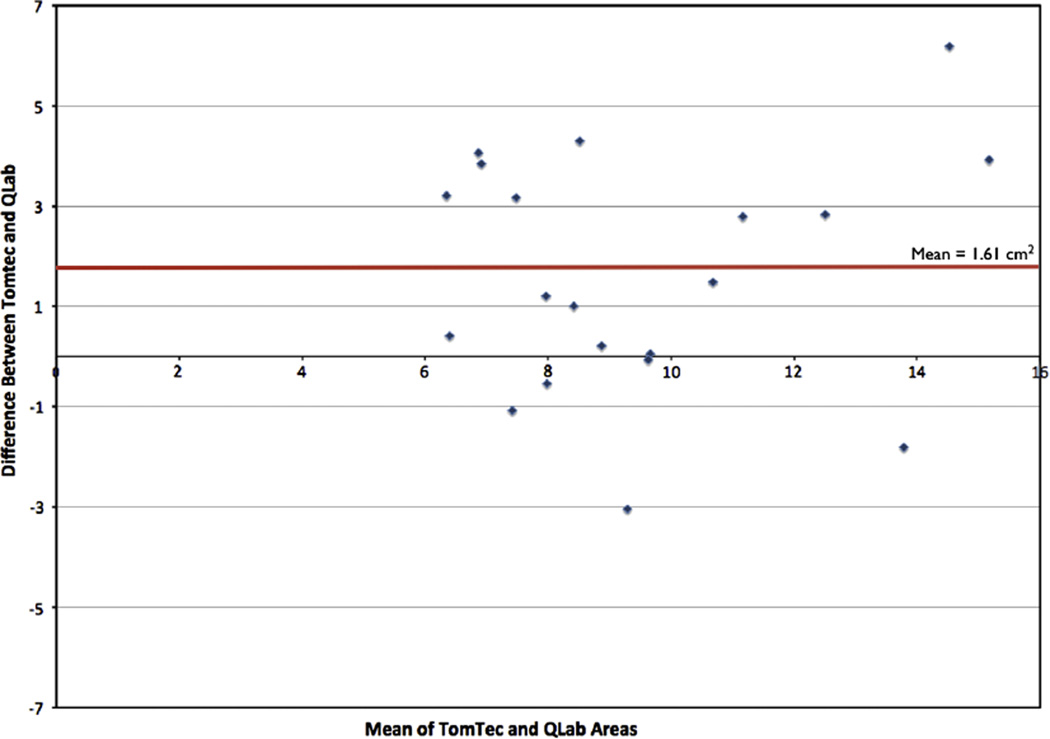
Measurements and main results: Volumetric data sets from 20 patients were acquired by 3D TEE and prospectively analyzed. Comparisons in annular geometry were made between groups based on the presence of TR. The QLab (Philips Medical Systems, Andover, MA) software package was used to calculate tricuspid annular area by both linear elliptical dimensions and planimetry. Further analyses were performed in the 4D Cardio-View (TomTec Corporation GmBH, Munich, Germany) and MATLAB (Natick, MA) software environments to accurately assess annular shape. It was found that patients with greater TR had an eccentrically dilated annulus with a larger annular area. Also, the area as measured by the linear ellipse method was overestimated as compared to the planimetry method. Furthermore, the irregular saddle-shaped geometry of the tricuspid annulus was confirmed through the mathematic model developed by the authors.
Conclusions: Three-dimensional TEE can be used to measure the tricuspid annular area in a clinically feasible fashion, with an eccentric dilation seen in patients with TR. The tricuspid annulus shape is complex, with annular high and low points, and annular area calculation based on linear measurements significantly overestimates 3D planimetered area.
Keywords: 3-dimensional transesophageal echocardiography; cardiac surgery; right ventricle; tricuspid annuloplasty; tricuspid regurgitation; tricuspidvalve.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Right heart three dimensional echocardiography: time for the limelight?J Cardiothorac Vasc Anesth. 2013 Aug;27(4):637-8. doi: 10.1053/j.jvca.2013.04.013. J Cardiothorac Vasc Anesth. 2013. PMID: 23849520 No abstract available.
References
-
- Sagie A, Schwammenthal E, Padial LR, et al. Determinants of functional tricuspid regurgitation in incomplete tricuspid valve closure: Doppler color flow study of 109 patients. J Am Coll Cardiol. 1994;24:446–453. - PubMed
-
- Matsunaga A, Duran CM. Progression of tricuspid regurgitation after repaired functional ischemic mitral regurgitation. Circulation. 2005;112:I453–I457. - PubMed
-
- Rogers JH, Bolling SF. Valve repair for functional tricuspid valve regurgitation: Anatomical and surgical considerations. Semin Thorac Cardiovasc Surg. 2010;22:84–89. - PubMed
-
- Anyanwu AC, Chikwe J, Adams DH. Tricuspid valve repair for treatment and prevention of secondary tricuspid regurgitation in patients undergoing mitral valve surgery. Curr Cardiol Rep. 2008;10:110–117. - PubMed
-
- Tang GH, David TE, Singh SK, et al. Tricuspid valve repair with an annuloplasty ring results in improved long-term outcomes. Circulation. 2006;114:I577–I581. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
