

The relationship between emergency department use and cost-related medication nonadherence among Medicare beneficiaries
- PMID: 23726522
- PMCID: PMC3812390
- DOI: 10.1016/j.annemergmed.2013.04.013
The relationship between emergency department use and cost-related medication nonadherence among Medicare beneficiaries
Abstract
Study objective: The objective of this study was to evaluate the relationship between self-reported cost-related nonadherence to prescription medications and emergency department (ED) utilization among Medicare beneficiaries. We hypothesized that persons who report cost-related medication nonadherence would have subsequent higher ED use.
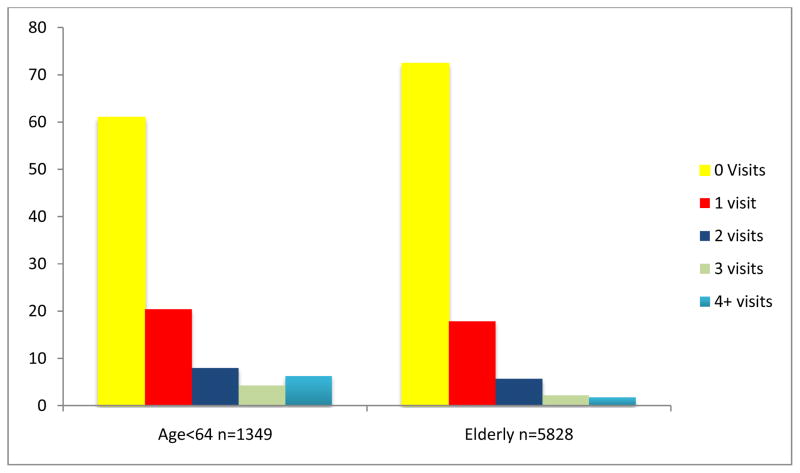
Methods: We conducted a retrospective cohort study of continuously enrolled Medicare beneficiaries in 2006 and 2007. We used multivariate logistic regression to evaluate the relationship between ED use and cost-related medication nonadherence. Our principal dependent variable was any ED visit within a 364-day period after an interview assessing cost-related medication nonadherence. Our principal independent variables both denoted cost-related medication nonadherence: mild cost-related medication nonadherence, defined as a reduction in dose or a delay in filling medications because of cost; and severe cost-related medication nonadherence, defined as not filling a medication at all because of cost.
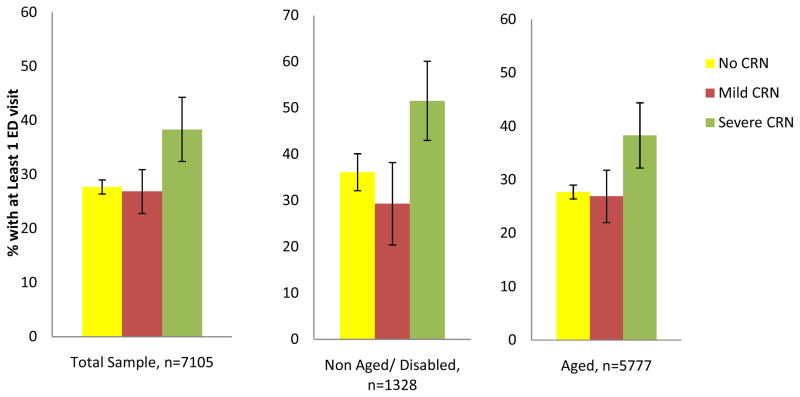
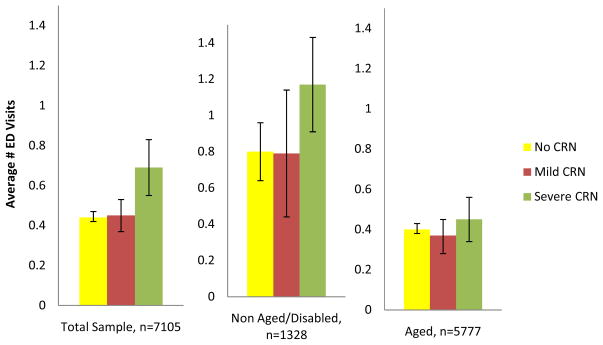
Results: Our sample consisted of 7,177 Medicare Current Beneficiary Survey respondents. Approximately 7.5% of respondents reported mild cost-related medication nonadherence only (n=541) and another 8.2% reported severe cost-related medication nonadherence (n=581). Disabled Medicare beneficiaries with severe cost-related medication nonadherence were more likely to have at least 1 ED visit (1.53; 95% confidence interval 1.03 to 2.26) compared with both disabled Medicare beneficiaries without cost-related medication nonadherence and elderly Medicare beneficiaries in all cost-related medication nonadherence categories.
Conclusion: Our results show an association between severe cost-related medication nonadherence and ED use. Disabled beneficiaries younger than 65 years who report severe cost-related medication nonadherence were more likely to have at least 1 ED visit, even when adjusting for other factors that affect utilization.
Copyright © 2013 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Centers for Medicare & Medicaid Services. [Accessed November 12, 2011];National Health Expenditure Accounts. http://www.cms.hhs.gov/NationalHealthExpendData/
-
- Stagnitti M. Average number of total (including refills) and unique prescriptions by select person characteristics, 2006. [Accessed March 3, 2012];MEPS Statistical Brief #245. 2009 May; http://meps.ahrq.gov/mepsweb/data_files/publications/st245/stat245.pdf.
-
- White House Domestic Policy Council. [Accessed February 29, 2012];Disability, Medicare and Prescription Drugs. http://clinton4.nara.gov/WH/EOP/nec/html/ParkMedicareReport000730.html.
-
- Foote SM, Hogan C. Disability Profile And Health Care Costs Of Medicare Beneficiaries Under Age sixty-five. Health Affairs. 2001;6:242–253. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
