

Comparison of survival among neoadjuvant chemoradiation responders, non-responders and patients receiving primary resection for locally advanced oesophageal squamous cell carcinoma: does neoadjuvant chemoradiation benefit all?
- PMID: 23728085
- PMCID: PMC3745136
- DOI: 10.1093/icvts/ivt216
Comparison of survival among neoadjuvant chemoradiation responders, non-responders and patients receiving primary resection for locally advanced oesophageal squamous cell carcinoma: does neoadjuvant chemoradiation benefit all?
Abstract
Objectives: While neoadjuvant chemoradiation followed by surgery has been shown to improve the survival of patients with locally advanced oesophageal cancer, it is not known whether neoadjuvant chemoradiation has a beneficial or harmful effect on the non-responders. We aimed to compare the outcomes among neoadjuvant chemoradiation responders, non-responders and patients receiving primary oesophagectomies for resectable locally advanced oesophageal squamous cell carcinoma.
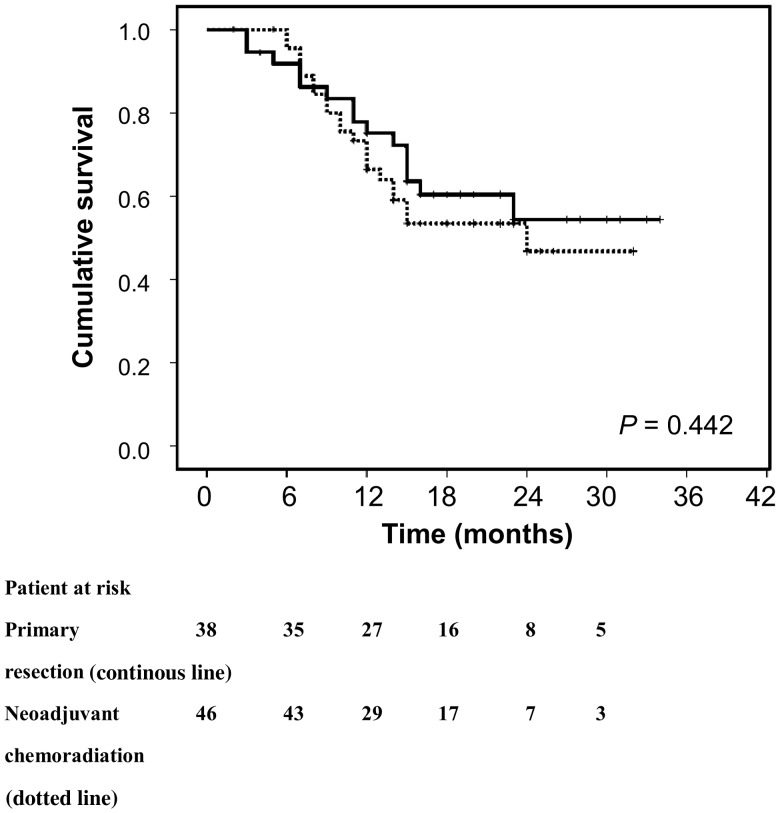
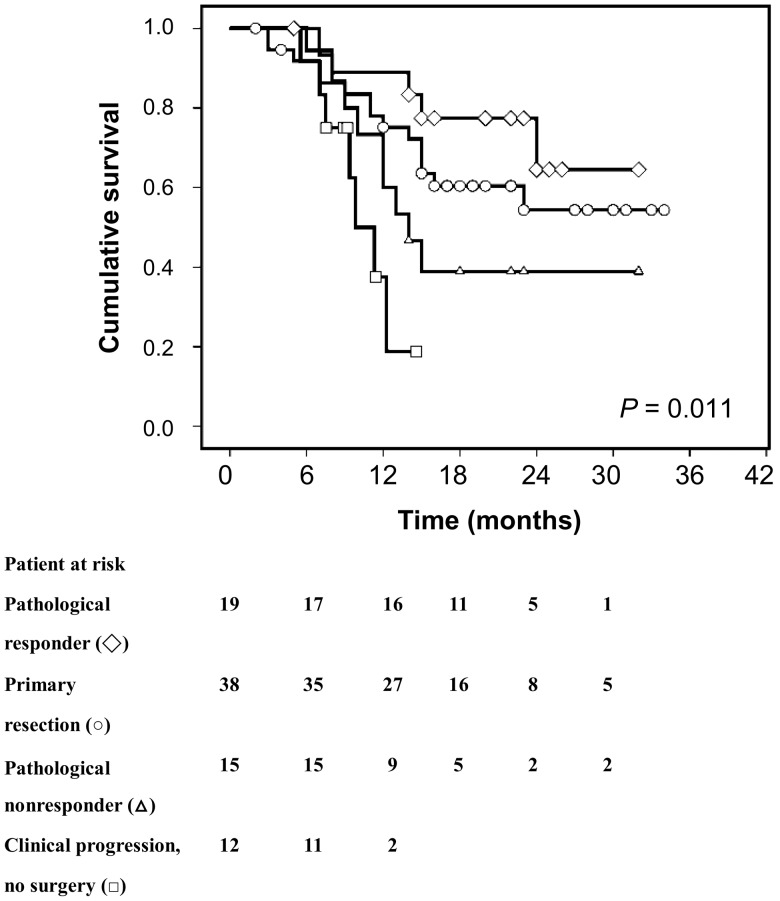
Methods: Eighty-four non-T1-2N0 oesophageal squamous cell carcinoma patients were included. Thirty-eight patients received primary resection and 46 patients received neoadjuvant chemoradiation. The overall survival of chemoradiation responders (<50% residual tumour), non-responders (>50% residual tumour and those who shifted to definitive chemoradiation instead of surgery due to tumour progression) and patients receiving primary resection were compared. Clinical parameters were also compared between responders and non-responders.
Results: There was no overall difference in survival between neoadjuvant chemoradiation and primary resection groups (2-year overall survival rates: 45.6 vs 54.3%, P = 0.442). In patients receiving neoadjuvant chemoradiation followed by surgery, pathological responders had significantly higher 2-year overall survival rates than non-responders (64.5 vs 38.9%, P = 0.043). While the pathological responders had the highest survival rate, clinicopathological non-responders (pathological non-responders and patients with tumour progression during the neoadjuvant chemoradiation period) demonstrated significantly worse outcomes than those receiving primary resection (32.0 vs 54.3%, P = 0.036). However, none of the clinical parameters, including blood profiles, images and baseline tumour characteristics, predicted the response to chemoradiation before treatment.
Conclusions: Neoadjuvant chemoradiation non-responders demonstrated no benefit and an even worse outcome compared with those receiving primary resection for locally advanced oesophageal squamous cell carcinoma. However, no significant clinical parameters could be implemented in the clinics to predict the response to neoadjuvant chemoradiation before treatment.
Keywords: Neoadjuvant chemoradiation; Oesophageal cancer; Squamous cell carcinoma; Survival.
Figures
Similar articles
-
Effects of Neoadjuvant Chemoradiotherapy on Pathological TNM Stage and Their Prognostic Significance for Surgically-treated Esophageal Squamous Cell Carcinoma.Anticancer Res. 2017 Oct;37(10):5639-5646. doi: 10.21873/anticanres.11999. Anticancer Res. 2017. PMID: 28982881
-
Role of neoadjuvant treatment in clinical T2N0M0 oesophageal cancer: results from a retrospective multi-center European study.Eur J Cancer. 2016 Mar;56:59-68. doi: 10.1016/j.ejca.2015.11.024. Epub 2016 Jan 23. Eur J Cancer. 2016. PMID: 26808298
-
Early surgery for failure after chemoradiation in operable thoracic oesophageal cancer. Analysis of the non-randomised patients in FFCD 9102 phase III trial: Chemoradiation followed by surgery versus chemoradiation alone.Eur J Cancer. 2015 Sep;51(13):1683-93. doi: 10.1016/j.ejca.2015.05.027. Epub 2015 Jul 7. Eur J Cancer. 2015. PMID: 26163097 Clinical Trial.
-
Current status of and perspectives regarding neoadjuvant chemoradiotherapy for locally advanced esophageal squamous cell carcinoma.Surg Today. 2016 Mar;46(3):261-7. doi: 10.1007/s00595-015-1144-0. Epub 2015 Mar 5. Surg Today. 2016. PMID: 25740123 Review.
-
Esophagectomy after chemoradiation: who and when to operate.Semin Thorac Cardiovasc Surg. 2012 Winter;24(4):288-93. doi: 10.1053/j.semtcvs.2012.10.005. Semin Thorac Cardiovasc Surg. 2012. PMID: 23465677 Review.
Cited by
-
The MRI radiomics signature can predict the pathologic response to neoadjuvant chemotherapy in locally advanced esophageal squamous cell carcinoma.Eur Radiol. 2024 Jan;34(1):485-494. doi: 10.1007/s00330-023-10040-4. Epub 2023 Aug 4. Eur Radiol. 2024. PMID: 37540319
-
Diffusion-weighted MRI and 18F-FDG PET/CT in assessing the response to neoadjuvant chemoradiotherapy in locally advanced esophageal squamous cell carcinoma.Radiat Oncol. 2021 Jul 19;16(1):132. doi: 10.1186/s13014-021-01852-z. Radiat Oncol. 2021. PMID: 34281566 Free PMC article.
-
A FDG-PET radiomics signature detects esophageal squamous cell carcinoma patients who do not benefit from chemoradiation.Sci Rep. 2020 Oct 19;10(1):17671. doi: 10.1038/s41598-020-74701-w. Sci Rep. 2020. PMID: 33077841 Free PMC article.
-
Role of surgery in multidisciplinary treatment strategies for locally advanced esophageal squamous cell carcinoma.Ann Gastroenterol Surg. 2020 Jun 22;4(5):490-497. doi: 10.1002/ags3.12364. eCollection 2020 Sep. Ann Gastroenterol Surg. 2020. PMID: 33005843 Free PMC article. Review.
-
Concurrent neoadjuvant chemoradiotherapy could improve survival outcomes for patients with esophageal cancer: a meta-analysis based on random clinical trials.Oncotarget. 2017 Mar 21;8(12):20410-20417. doi: 10.18632/oncotarget.14669. Oncotarget. 2017. PMID: 28099899 Free PMC article. Review.
References
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–52. doi:10.1056/NEJMra035010. - DOI - PubMed
-
- Hsu PK, Wang BY, Huang CS, Wu YC, Hsu WH. Prognostic factors for post-recurrence survival in esophageal squamous cell carcinoma patients with recurrence after resection. J Gastrointest Surg. 2011;15:558–65. doi:10.1007/s11605-011-1458-1. - DOI - PubMed
-
- Tepper J, Krasna MJ, Niedzwiecki N, Hollis D, Reed CE, Goldberg R, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol. 2008;26:1086–92. doi:10.1200/JCO.2007.12.9593. - DOI - PMC - PubMed
-
- Van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–84. doi:10.1056/NEJMoa1112088. - DOI - PubMed
-
- Burmeister BH, Smithers BM, Gebski V, Fitzgerald L, Simes RJ, Devitt P, et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomised controlled phase III trial. Lancet Oncol. 2005;6:659–68. doi:10.1016/S1470-2045(05)70288-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
