

Cognitive rehabilitation for attention deficits following stroke
- PMID: 23728639
- PMCID: PMC6464967
- DOI: 10.1002/14651858.CD002842.pub2
Cognitive rehabilitation for attention deficits following stroke
Update in
-
Cognitive rehabilitation for attention deficits following stroke.Cochrane Database Syst Rev. 2019 Nov 10;2019(11):CD002842. doi: 10.1002/14651858.CD002842.pub3. Cochrane Database Syst Rev. 2019. PMID: 31706263 Free PMC article.
Abstract
Background: Many survivors of stroke complain about attentional impairments, such as diminished concentration and mental slowness. However, the effectiveness of cognitive rehabilitation for improving these impairments is uncertain.
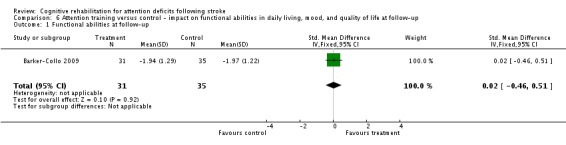
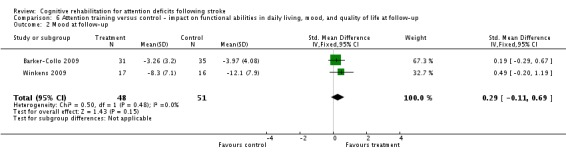
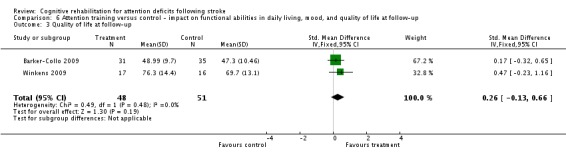
Objectives: To determine whether (1) people receiving attentional treatment show better outcomes in their attentional functions than those given no treatment or treatment as usual, and (2) people receiving attentional treatment techniques have a better functional recovery, in terms of independence in activities of daily living, mood and quality of life, than those given no treatment or treatment as usual.
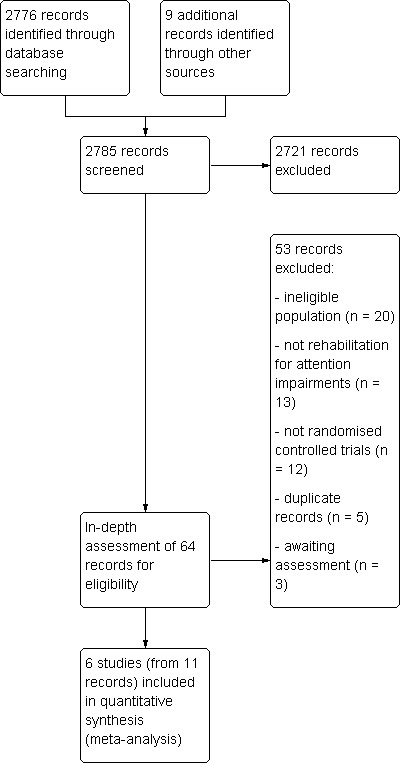
Search methods: We searched the Cochrane Stroke Group Trials Register (October 2012), Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library October 2012), MEDLINE (1948 to October 2012), EMBASE (1947 to October 2012), CINAHL (1981 to October 2012), PsycINFO (1806 to October 2012), PsycBITE and REHABDATA (searched October 2012) and ongoing trials registers. We screened reference lists and tracked citations using Scopus.
Selection criteria: We included randomised controlled trials (RCTs) of cognitive rehabilitation for impairments of attention for people with stroke. The primary outcome was measures of global attentional functions, and secondary outcomes were measures of attention domains, functional abilities, mood and quality of life.
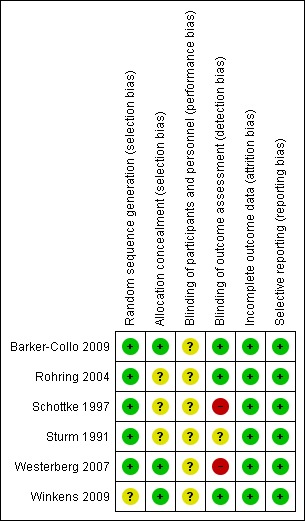
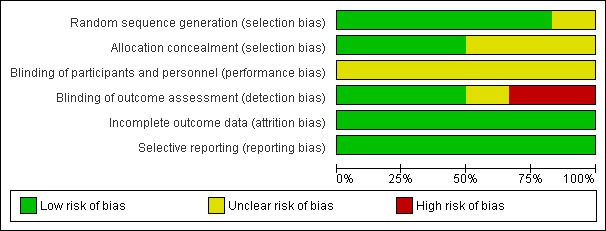
Data collection and analysis: Two review authors independently selected trials, extracted data and assessed trial quality.
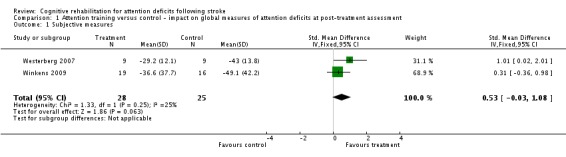
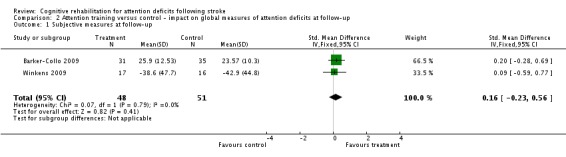
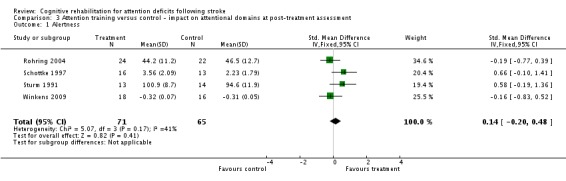
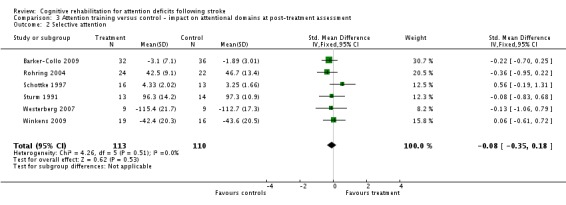
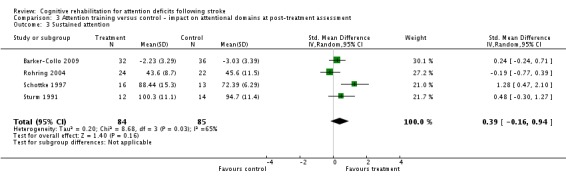
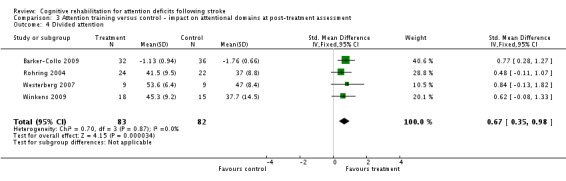
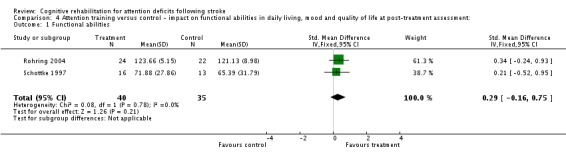
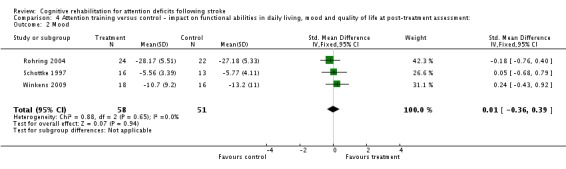
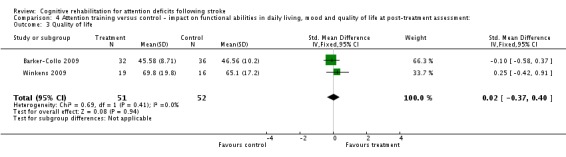
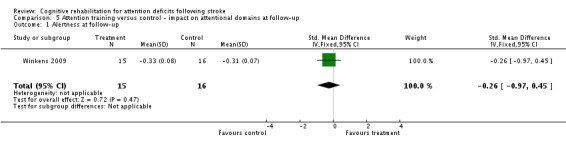
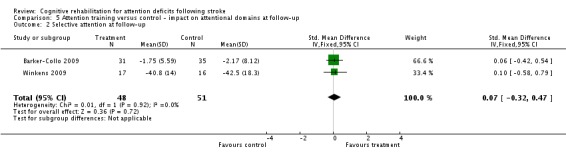
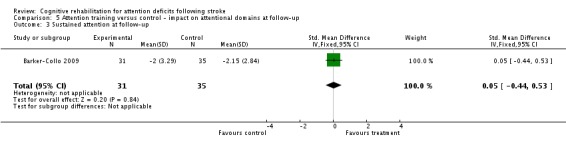
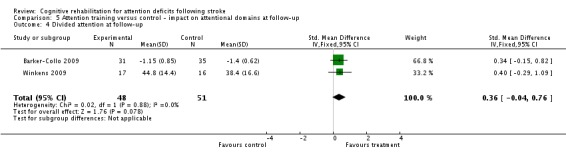
Main results: We included six RCTs with 223 participants. All six RCTs compared cognitive rehabilitation with a usual care control. Meta-analyses demonstrated no statistically significant effect of cognitive rehabilitation for persisting effects on global measures of attention (two studies, 99 participants; standardised mean difference (SMD) 0.16, 95% confidence interval (CI) -0.23 to 0.56; P value = 0.41), standardised attention assessments (two studies, 99 participants; P value ≥ 0.08) or functional outcomes (two studies, 99 participants; P value ≥ 0.15). In contrast, a statistically significant effect was found in favour of cognitive rehabilitation when compared with control for immediate effects on measures of divided attention (four studies, 165 participants; SMD 0.67, 95% CI 0.35 to 0.98; P value < 0.0001) but no significant effects on global attention (two studies, 53 participants; P value = 0.06), other attentional domains (six studies, 223 participants; P value ≥ 0.16) or functional outcomes (three studies, 109 participants; P value ≥ 0.21).Thus there was limited evidence that cognitive rehabilitation may improve some aspects of attention in the short term, but there was insufficient evidence to support or refute the persisting effects of cognitive rehabilitation on attention, or on functional outcomes in either the short or long term.
Authors' conclusions: The effectiveness of cognitive rehabilitation remains unconfirmed. The results suggest there may be a short-term effect on attentional abilities, but future studies need to assess the persisting effects and measure attentional skills in daily life. Trials also need to have higher methodological quality and better reporting.
Conflict of interest statement
None known.
Figures
Update of
-
Cognitive rehabilitation for attention deficits following stroke.Cochrane Database Syst Rev. 2000;(4):CD002842. doi: 10.1002/14651858.CD002842. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2013 May 31;(5):CD002842. doi: 10.1002/14651858.CD002842.pub2. PMID: 11034773 Updated.
References
References to studies included in this review
-
- Barker‐Collo SL, Feigin VL, Lawes CM, Parag V, Senior H, Rodgers A. Reducing attention deficits after stroke using attention process training: a randomized controlled trial. Stroke 2009;40:3293‐8. - PubMed
-
- Röhring S, Kulke H, Reulbach U, Peetz H, Schupp W. Effectivity of a neuropsychological training in attention functions by a teletherapeutic setting. Neurologie und Rehabilitation 2004;10(5):239‐46.
-
- Schottke H. Rehabilitation of attention deficits after stroke ‐ efficacy of a Neuropsychological training program for attention deficits [Rehabilitation von Aufmerksamkeitsstörungen nach einem Schlaganfall ‐ Effektivität eines verhaltensmedizinisch‐neuropsychologischen Aufmerksamkeitstrainings]. Verhaltenstherapie 1997;7:21‐3.
-
- Sturm W, Willmes K. Efficacy of a reaction training on various attentional and cognitive functions in stroke patients. Neuropsychological Rehabilitation 1991;1:259‐80.
-
- Westerberg H, Jacobaeus H, Hirvikoski T, Clevberger P, Ostensson ML, Bartfai A, et al. Computerized working memory training after stroke ‐ a pilot study. Brain Injury 2007;21(1):21‐9. - PubMed
References to studies excluded from this review
-
- Aivazian TA, Zaitsev VP, Taravkova IA, Gorbunov FE, Maslovskaia SG, Strelnikov AV. The relaxation psychotherapy of patients with cerebrovascular diseases: its efficacy and predictors. Voprosy Kurortologii, Fizioterapii, i Lechebnoi Fizicheskoi Kultury 1994;2:2‐4. - PubMed
-
- Akinwuntan AE, Devos H, Verheyden G, Baten G, Kiekens C, Feys H, et al. Retraining moderately impaired stroke survivors in driving‐related visual attention skills. Topics in Stroke Rehabilitation 2010;17:328–36. - PubMed
-
- Boman IL, Lindstedt M, Hemmingsson H, Bartfai A. Cognitive training in home environment. Brain Injury 2004;18(10):985‐95. - PubMed
-
- Brainin M. Austrian Polyintervention Study to Prevent Cognitive Decline After Ischemic Stroke (ASPIS). clinicaltrials.gov/show/NCT01109836 (accessed 12 April 2013).
-
- Bunketorp Kall L. The effects of a rhythm and music‐based therapy program and therapeutic riding in late recovery phase following stroke. clinicaltrials.gov/ct2/show/NCT01372059 (accessed 12 April 2013). - PMC - PubMed
References to studies awaiting assessment
-
- Flynn A. Investigation into whether psychology led cognitive rehabilitation of attentional and visio‐spatial skills improves performance in these areas beyond spontaneous recovery. National Research Register (N0280012930) (accessed October 2012).
-
- Matz K, Teuschl Y, Eckhardt R, Herbst A, Dachenhausen A, Brainin M. Cognitive training in patients with first lacunar stroke ‐ a randomized pilot trial for the prevention of post‐stroke cognitive decline. Cerebrovascular Diseases 2007;23 Suppl 2:42.
References to ongoing studies
-
- Frommelt P. Neuropsychological rehabilitation: Modular cognitive retraining versus compensatory skills training. ISRCTN Register (ISRCTN45171788) (accessed October 2012).
Additional references
-
- Barker‐Collo S, Feigin V. The impact of neuropsychological deficits on functional stroke outcomes. Neuropsychology Review 2006;16:53‐64. - PubMed
-
- Barker‐Collo S, Feigin VL, Parag V, Lawes CMM, Senior H. Auckland Stroke Outcomes Study Part 2: cognition and functional outcomes 5 years poststroke. Neurology 2010;75:1608‐18. - PubMed
-
- Broadbent DE, Cooper PF, FitzGerald P, Parkes KR. The Cognitive Failures Questionnaire (CFQ) and its correlates. British Journal of Clinical Psychology 1982;21:1‐16. - PubMed
-
- Cappa SF, Benke T, Clarke S, Rossi B, Stemmer B, Heugten CM. EFNS guidelines on cognitive rehabilitation: report of an EFNS task force. European Journal of Neurology 2005;12:665‐80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical