

Home- or community-based programmes for treating malaria
- PMID: 23728693
- PMCID: PMC6532579
- DOI: 10.1002/14651858.CD009527.pub2
Home- or community-based programmes for treating malaria
Abstract
Background: Malaria is an important cause of morbidity and mortality, in particular among children and pregnant women in sub-Saharan Africa. Prompt access to diagnosis and treatment with effective antimalarial drugs is a central component of the World Health Organization's (WHO) strategy for malaria control. Home- or community-based programmes for managing malaria are one strategy that has been proposed to overcome the geographical barrier to malaria treatment.
Objectives: To evaluate home- and community-based management strategies for treating malaria.
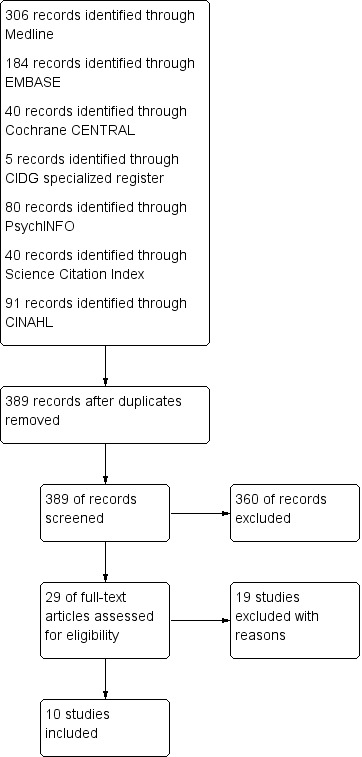
Search methods: We searched the Cochrane Central Register of Controlled Trials published in The Cochrane Library; MEDLINE; EMBASE; Science Citation Index; PsycINFO/LIT; CINAHL; WHO clinical trial registry platform; and the metaRegister of Controlled Trials up to September 2012.
Selection criteria: Randomized controlled trials (RCTs) and non-RCTs that evaluated the effects of a home- or community-based programme for treating malaria in a malaria endemic setting.
Data collection and analysis: Two authors independently screened and selected studies, extracted data, and assessed the risk of bias. Where possible the effects of interventions are compared using risk ratios (RR), and presented with 95% confidence intervals (CI). The quality of the evidence was assessed using the GRADE approach.
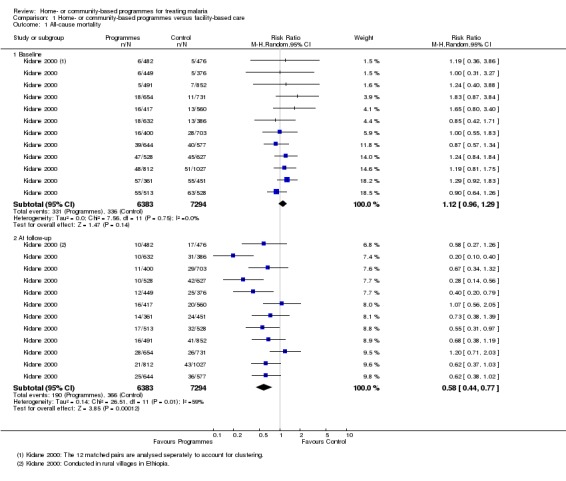
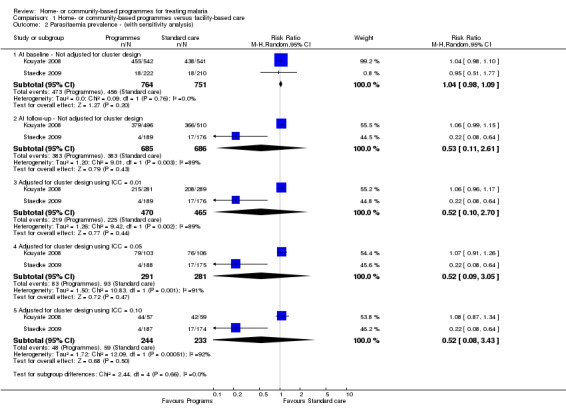
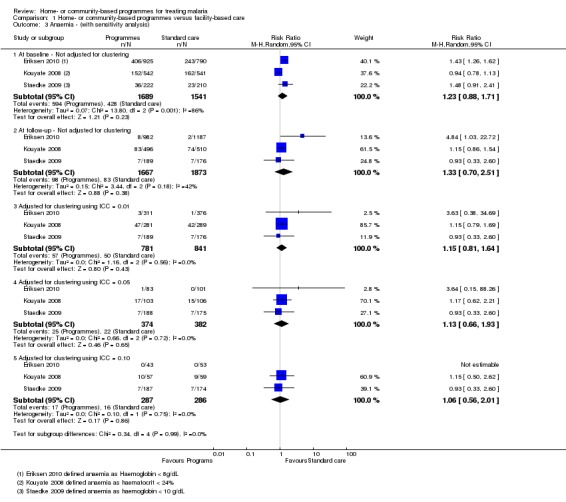
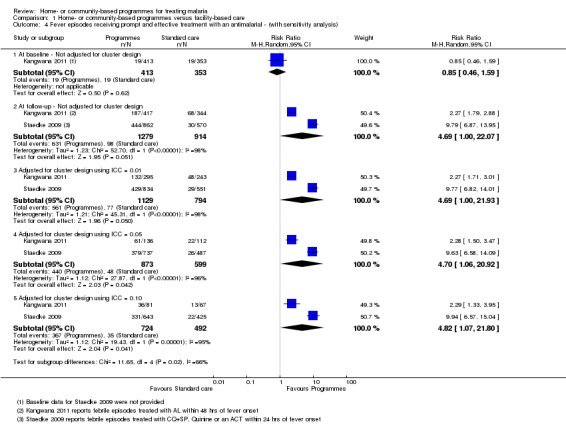
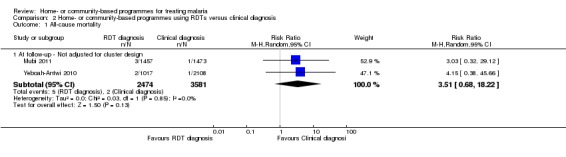
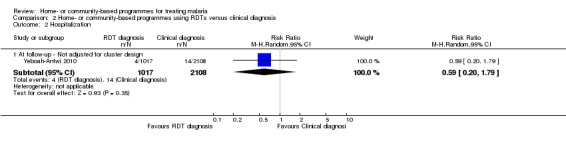
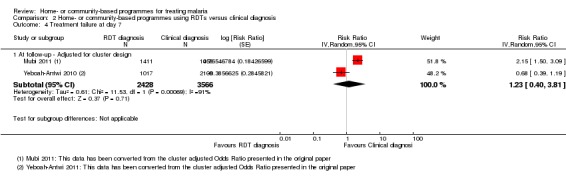
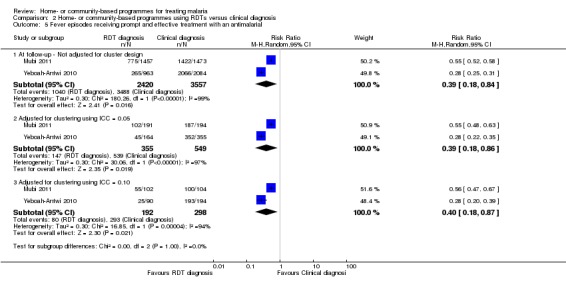
Main results: We identified 10 trials that met the inclusion criteria. The interventions involved brief training of basic-level health workers or mothers, and most provided the antimalarial for free or at a highly subsidized cost. In eight of the studies, fevers were treated presumptively without parasitological confirmation with microscopy or a rapid diagnostic test (RDT). Two studies trained community health workers to use RDTs as a component of community management of fever.Home- or community-based strategies probably increase the number of people with fever who receive an appropriate antimalarial within 24 hours (RR 2.27, 95% CI 1.79 to 2.88 in one trial; RR 9.79, 95% CI 6.87 to 13.95 in a second trial; 3099 participants, moderate quality evidence). They may also reduce all-cause mortality, but to date this has only been demonstrated in rural Ethiopia (RR 0.58, 95% CI 0.44 to 0.77, one trial, 13,677 participants, moderate quality evidence).Hospital admissions in children were reported in one small trial from urban Uganda, with no effect detected (437 participants, very low quality evidence). No studies reported on severe malaria. For parasitaemia prevalence, the study from urban Uganda demonstrated a reduction in community parasite prevalence (RR 0.22, 95% CI 0.08 to 0.64, 365 participants), but a second study in rural Burkina Faso did not (1006 participants). Home- or community-based programmes may have little or no effect on the prevalence of anaemia (three trials, 3612 participants, low quality evidence). None of the included studies reported on adverse effects of using home- or community-based programmes for treating malaria.In two studies which trained community health workers to only prescribe antimalarials after a positive RDT, prescriptions of antimalarials were reduced compared to the control group where community health workers used clinical diagnosis (RR 0.39, 95% CI 0.18 to 0.84, two trials, 5944 participants, moderate quality evidence). In these two studies, mortality and hospitalizations remained very low in both groups despite the lower use of antimalarials (two trials, 5977 participants, low quality evidence).
Authors' conclusions: Home- or community-based interventions which provide antimalarial drugs free of charge probably improve prompt access to antimalarials, and there is moderate quality evidence from rural Ethiopia that they may impact on childhood mortality when implemented in appropriate settings.Programmes which treat all fevers presumptively with antimalarials lead to overuse antimalarials, and potentially undertreat other causes of fever such as pneumonia. Incorporating RDT diagnosis into home- or community-based programmes for malaria may help to reduce this overuse of antimalarials, and has been shown to be safe under trial conditions.
Conflict of interest statement
None known.
Figures



Update of
References
References to studies included in this review
-
- Kidane G, Morrow RH. Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomised trial. Lancet 2000;356(9229):550‐5. - PubMed
References to studies excluded from this review
-
- Ajayi IO, Falade CO, Kale OO. An assessment of accuracy of mothers' presumptive diagnosis of fever at home in southwest Nigeria: evidence for switch to parasite‐based diagnostic test. East African Journal of Public Health 2009;6(3):229‐34. - PubMed
References to ongoing studies
-
- Ohnmar. Cluster randomized trial on the use of community volunteers to improve early diagnosis and appropriate treatment of malaria in Bago Division, Myanmar. Australian New Zealand Clinical Trials Registry Accessed 25 September 2012:ACTRN12610000706077.
Additional references
-
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction‐GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. - PubMed
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Chichester: John Wiley & Sons, Ltd., 2008.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous