

Desquamative interstitial pneumonia: an analytic review with an emphasis on aetiology
- PMID: 23728865
- PMCID: PMC9487388
- DOI: 10.1183/09059180.00005812
Desquamative interstitial pneumonia: an analytic review with an emphasis on aetiology
Abstract
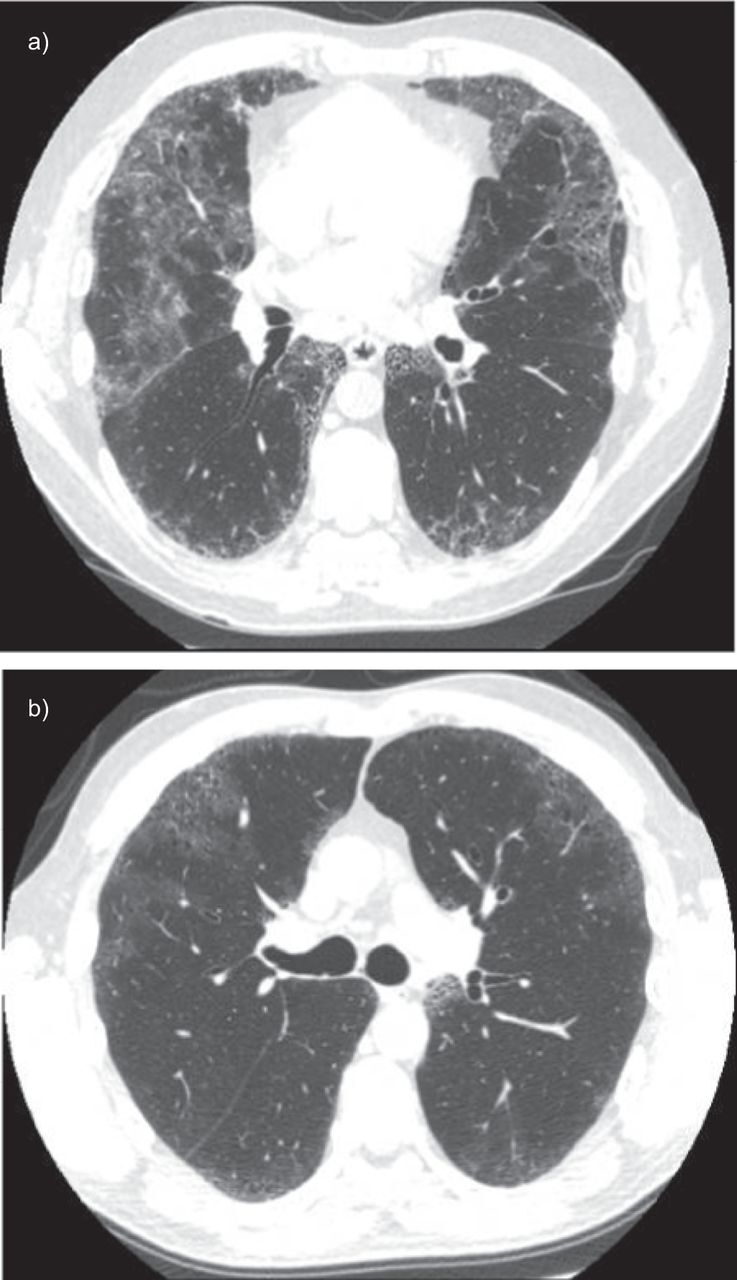
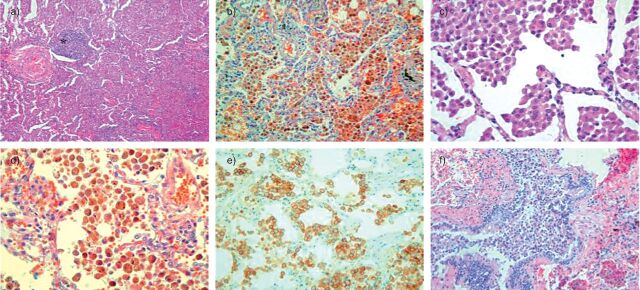
Desquamative interstitial pneumonia (DIP) is characterised by the accumulation of numerous pigmented macrophages within most of the distal airspace of the lung and, sometimes, the presence of giant cells. Diagnosis of DIP is not easy and requires surgical lung biopsy. DIP is usually associated with tobacco smoke. However, the association between smoking and DIP is less robust than that with respiratory bronchiolitis with interstitial lung disease or pulmonary Langerhans' cell histiocytosis; approximately 10-42% of patients with DIP are nonsmokers. DIP can also occur in patients following exposure to certain inhaled toxins (occupational exposure) and drugs, and may occur in the context of certain viral illnesses and autoimmune diseases. In the context of DIP, occupational exposure should be systematically investigated.
Keywords: Giant cell; interstitial lung disease; macrophages; occupational lung disease; surgical lung biopsy; tobacco.
Conflict of interest statement
None declared.
Figures
References
-
- Liebow AA, Steer A, Billingsley JG. Desquamative interstitial pneumonia. Am J Med 1965; 39: 369–404. - PubMed
-
- Liebow AA, Carrington CB. The interstitial pneumonias. In: Simon M, Potchen EJ, LeMay M, eds. Frontiers of pulmonary radiology. 1st Edn. New York, Grune and Stratton, 1969; pp. 102–141.
-
- Tubbs RR, Benjamin SP, Reich NE, et al. . Desquamative interstitial pneumonitis. Cellular phase of fibrosing alveolitis. Chest 1977; 72: 159–165. - PubMed
-
- American Thoracic Society., European Respiratory Society. International multidisciplinary consensus. Classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002; 165: 277–304. - PubMed
-
- Yousem SA, Colby TV, Gaensler EA. Respiratory bronchiolitis-associated interstitial lung disease and its relationship to desquamative interstitial pneumonia. Mayo Clin Proc 1989; 64: 1373–1380. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical