

Accelerated partial-breast irradiation using intensity-modulated proton radiotherapy: do uncertainties outweigh potential benefits?
- PMID: 23728947
- PMCID: PMC3755395
- DOI: 10.1259/bjr.20130176
Accelerated partial-breast irradiation using intensity-modulated proton radiotherapy: do uncertainties outweigh potential benefits?
Abstract
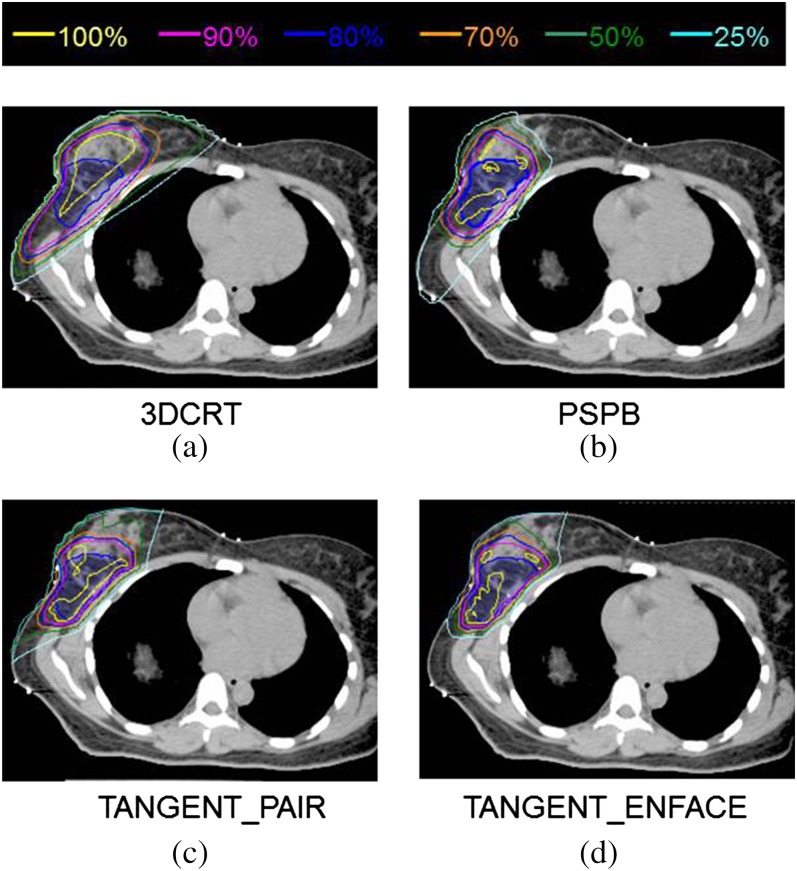
Objective: Passive scattering proton beam (PSPB) radiotherapy for accelerated partial-breast irradiation (APBI) provides superior dosimetry for APBI three-dimensional conformal photon radiotherapy (3DCRT). Here we examine the potential incremental benefit of intensity-modulated proton radiotherapy (IMPT) for APBI and compare its dosimetry with PSPB and 3DCRT.
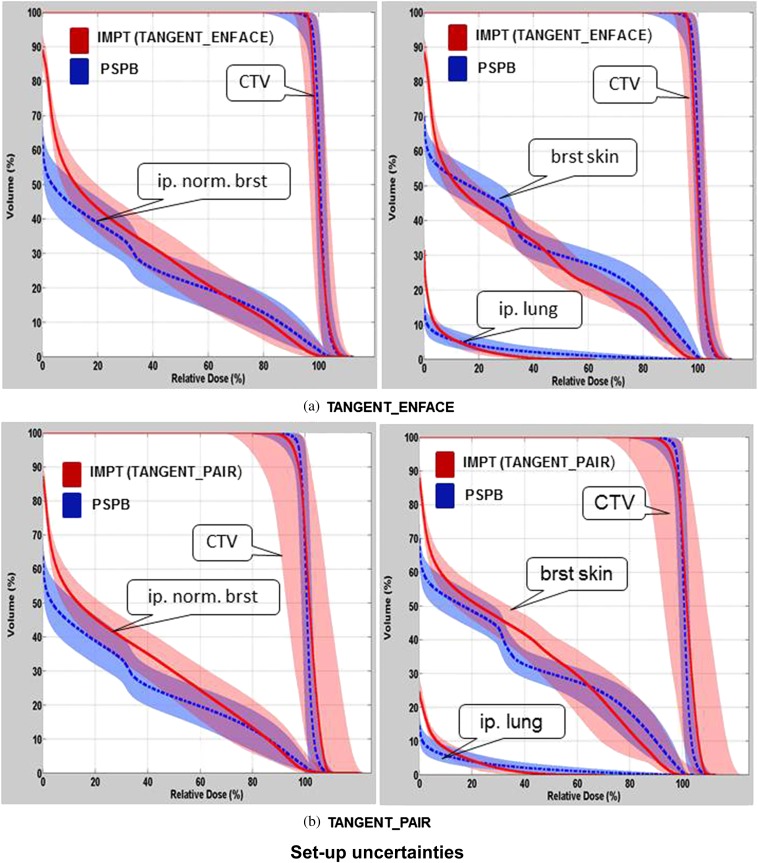
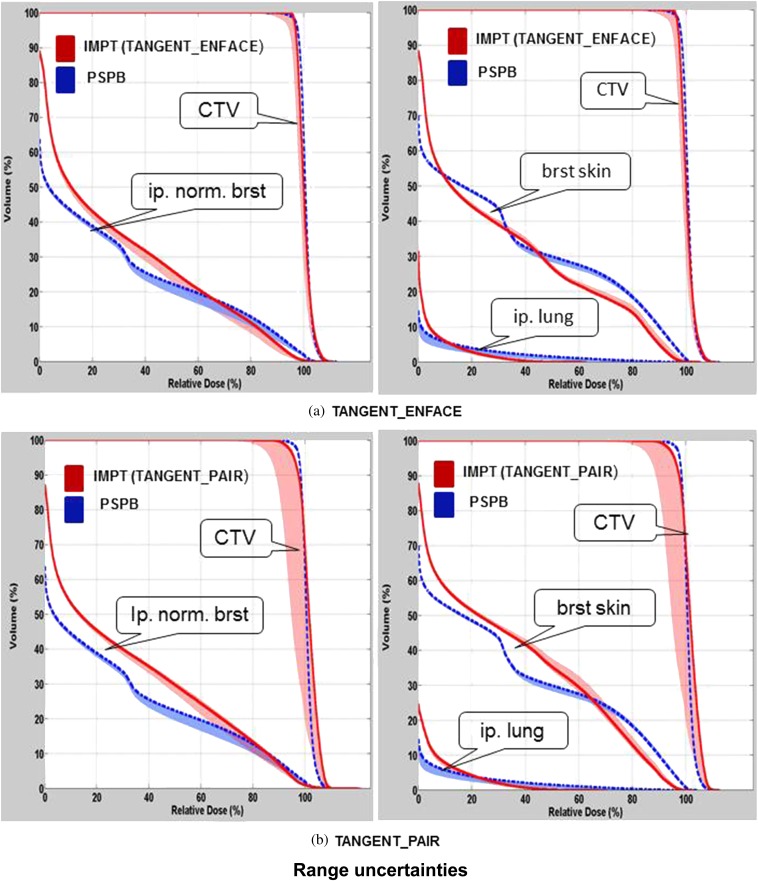
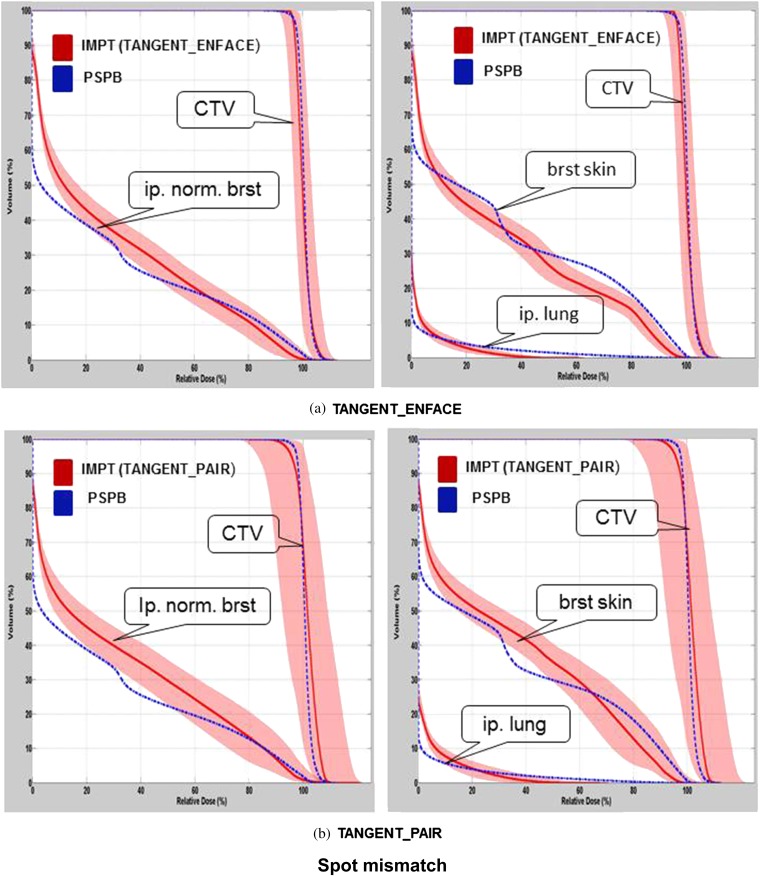
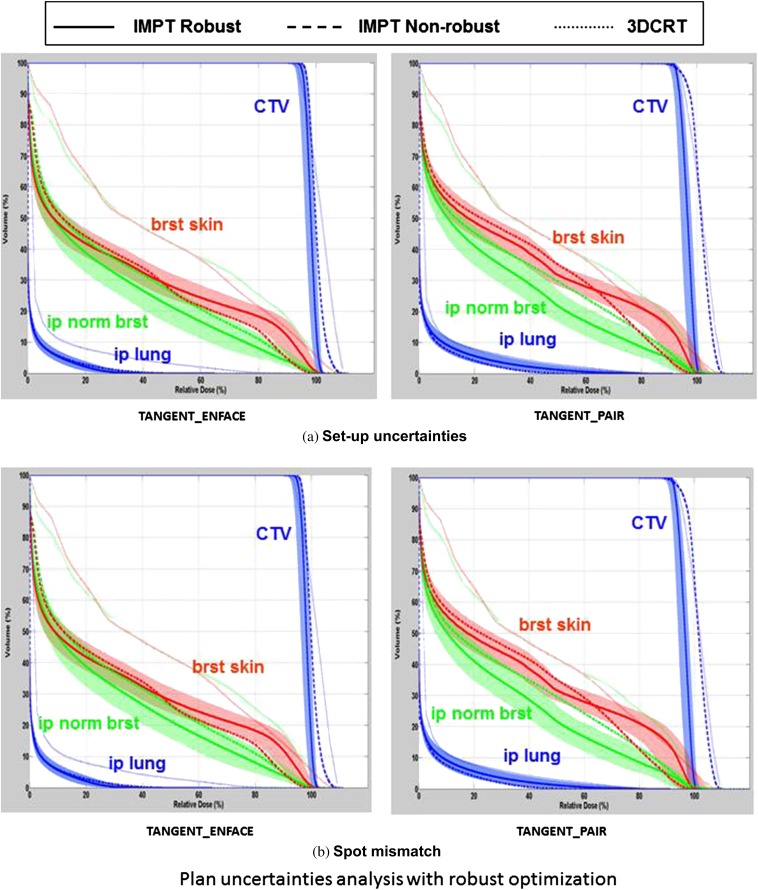
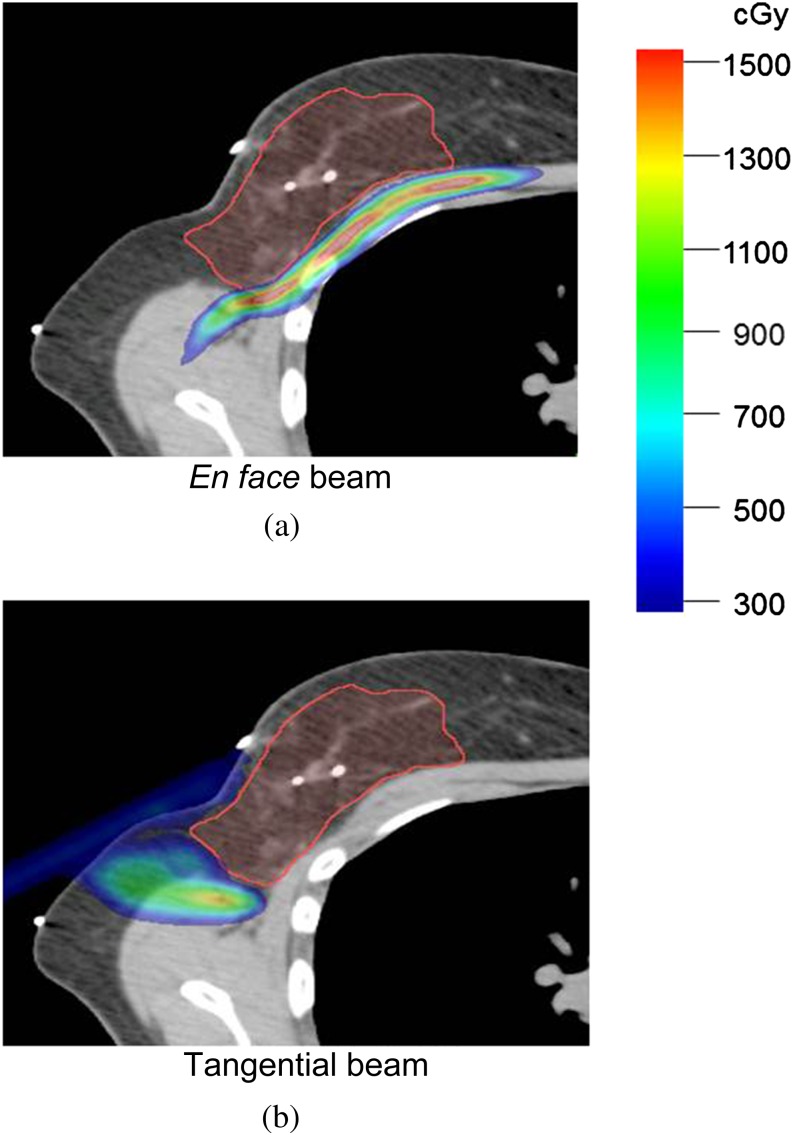
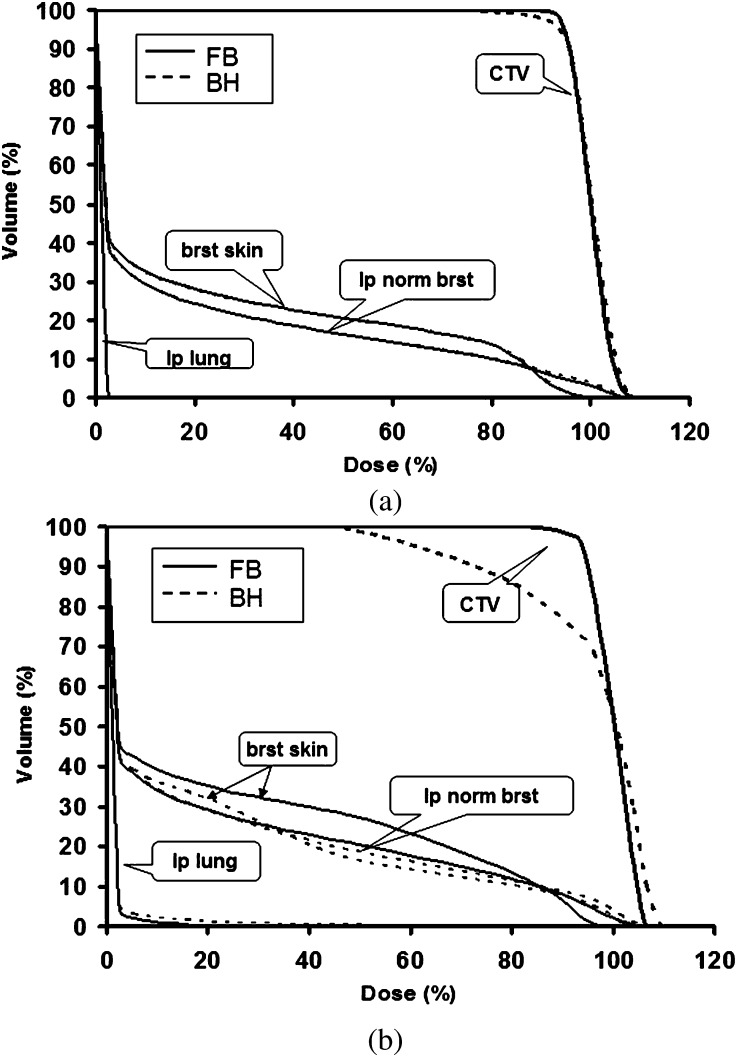
Methods: Two theoretical IMPT plans, TANGENT_PAIR and TANGENT_ENFACE, were created for 11 patients previously treated with 3DCRT APBI and were compared with PSPB and 3DCRT plans for the same CT data sets. The impact of range, motion and set-up uncertainties as well as scanned spot mismatching between fields of IMPT plans was evaluated.
Results: IMPT plans for APBI were significantly better regarding breast skin sparing (p<0.005) and other normal tissue sparing than 3DCRT plans (p<0.01) with comparable target coverage (p=ns). IMPT plans were statistically better than PSPB plans regarding breast skin (p<0.002) and non-target breast (p<0.007) in higher dose regions but worse or comparable in lower dose regions. IMPT plans using TANGENT_ENFACE were superior to that using TANGENT_PAIR in terms of target coverage (p<0.003) and normal tissue sparing (p<0.05) in low-dose regions. IMPT uncertainties were demonstrated for multiple causes. Qualitative comparison of dose-volume histogram confidence intervals for IMPT suggests that numeric gains may be offset by IMPT uncertainties.
Conclusion: Using current clinical dosimetry, PSPB provides excellent dosimetry compared with 3DCRT with fewer uncertainties compared with IMPT.
Advances in knowledge: As currently delivered in the clinic, PSPB planning for APBI provides as good or better dosimetry than IMPT with less uncertainty.
Figures
References
-
- Smith BD, Arthur DW, Buchholz TA, Haffty BG, Hahn CA, Hardenbergh PH, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). Int J Radiat Oncol Biol Phys 2009;74:987–1001 - PubMed
-
- Whelan TJ, Olivotto I, Parpia S, Berrang T, Kim D, Kong I, et al. Interim toxicity results from RAPID: a randomized trial of accelerated partial breast irradiation (APBI) using 3D conformal external beam radiation therapy (3DCRT). Int J Radiat Oncol Biol Phys 2013;85:21–2 - PubMed
-
- Rusthoven KE, Carter DL, Howell K, Kercher JM, Henkenberns P, Hunter KL, et al. Accelerated partial-breast intensity-modulated radiotherapy results in improved dose distribution when compared with three-dimensional treatment-planning techniques. Int J Radiat Oncol Biol Phys 2008;70:296–302 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
