

Identification of patients at risk for hereditary colorectal cancer
- PMID: 23730221
- PMCID: PMC3423884
- DOI: 10.1055/s-0032-1313777
Identification of patients at risk for hereditary colorectal cancer
Abstract
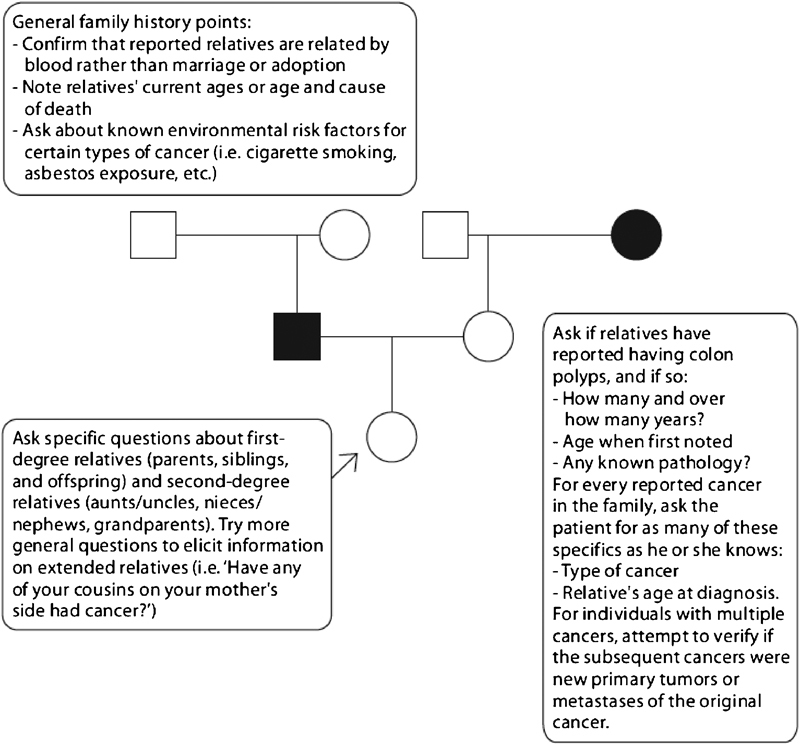
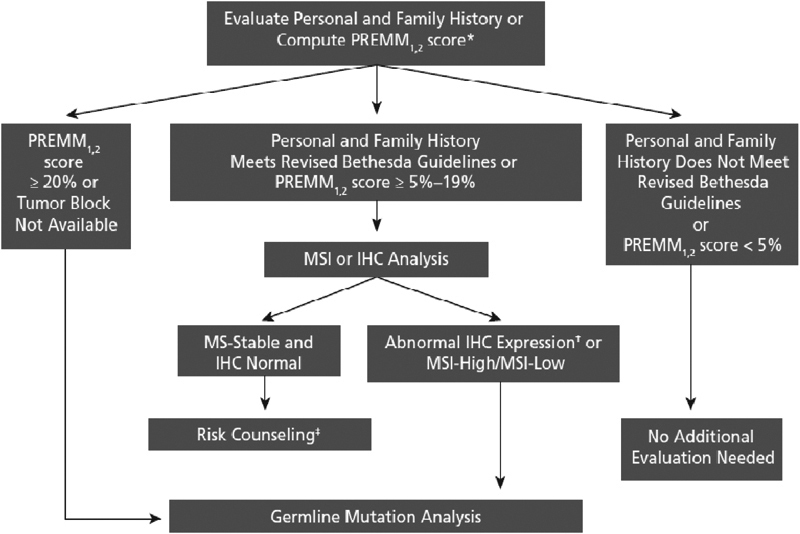
Diagnosis of hereditary colorectal cancer syndromes requires clinical suspicion and knowledge of such syndromes. Lynch syndrome is the most common cause of hereditary colorectal cancer. Other less common causes include familial adenomatous polyposis (FAP), Peutz-Jeghers syndrome (PJS), juvenile polyposis syndrome, and others. There have been a growing number of clinical and molecular tools used to screen and test at risk individuals. Screening tools include diagnostic clinical criteria, family history, genetic prediction models, and tumor testing. Patients who are high risk based on screening should be referred for genetic testing.
Keywords: Lynch syndrome; Peutz-Jeghers syndrome; familial adenomatous polyposis.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun M J. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–249. - PubMed
-
- Mecklin J P. Frequency of hereditary colorectal carcinoma. Gastroenterology. 1987;93(5):1021–1025. - PubMed
-
- Ponz de Leon M, Sassatelli R, Sacchetti C, Zanghieri G, Scalmati A, Roncucci L. Familial aggregation of tumors in the three-year experience of a population-based colorectal cancer registry. Cancer Res. 1989;49(15):4344–4348. - PubMed
-
- Samowitz W S, Curtin K, Lin H H. et al.The colon cancer burden of genetically defined hereditary nonpolyposis colon cancer. Gastroenterology. 2001;121(4):830–838. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
