

Abnormal Neurodevelopmental Outcomes are Common in Children with Transient Congenital Hyperinsulinism
- PMID: 23730298
- PMCID: PMC3657691
- DOI: 10.3389/fendo.2013.00060
Abnormal Neurodevelopmental Outcomes are Common in Children with Transient Congenital Hyperinsulinism
Abstract
Introduction: Neuroglycopenia is recognized to be associated with abnormal neurodevelopmental outcomes in 26-44% of children with persistent congenital hyperinsulinism (P-CHI). The prevalence of abnormal neurodevelopment in transient CHI (T-CHI) is not known. We have aimed to investigate abnormal neurodevelopment and associated factors in T-CHI and P-CHI.
Materials and methods: A cohort of children with CHI (n = 67, age 2.5-5 years) was assessed at follow-up review and noted to have normal or abnormal (mild or severe) neurodevelopmental outcomes for the domains of speech and language, motor, and vision. Children were classified as P-CHI (n = 33), if they had undergone surgery or remained on medical therapy, or T-CHI (n = 34), if medical treatment for hypoglycemia was stopped.
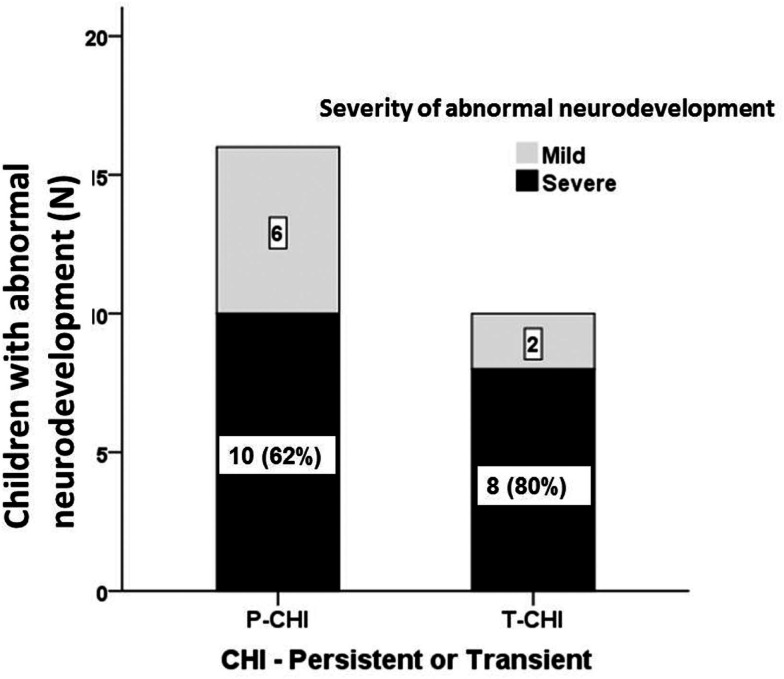
Results: Overall, abnormal neurodevelopment was present in 26 (39%) children with CHI, of whom 18 (69%) were severe. Importantly, the incidence of abnormal neurodevelopment in T-CHI was similar to that in P-CHI (30 vs. 47% respectively, p = 0.16). The prevalence of severe abnormal neurodevelopment in speech, motor, and vision domains was similar in both T-CHI and P-CHI children. For this cohort, we found that the severity of disease [based upon maximal diazoxide dose (odds ratio 95% confidence intervals) 1.3 (1.1; 1.5), p = 0.03], and early presentation of CHI <7 days following birth [5.9 (1.3; 27.8), p = 0.02] were significantly associated with abnormal neurodevelopment. There was no significant association with gender, genotype, or the histopathological basis of CHI.
Conclusion: Abnormal neurodevelopment was evident in one third of children with both T-CHI and P-CHI, early presentation and severe CHI being risk factors. Early recognition and rapid correction of hypoglycemia are advocated to avoid abnormal neurodevelopment in children with CHI.
Keywords: congenital hyperinsulinism; developmental delay; hypoglycemia; neurodevelopment; neurological outcome; seizures; transient congenital hyperinsulinism.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources