

A Randomized, Controlled Trial Comparing Autologous Matrix-Induced Chondrogenesis (AMIC®) to Microfracture: Analysis of 1- and 2-Year Follow-Up Data of 2 Centers
- PMID: 23730377
- PMCID: PMC3664447
- DOI: 10.2174/1874325001307010133
A Randomized, Controlled Trial Comparing Autologous Matrix-Induced Chondrogenesis (AMIC®) to Microfracture: Analysis of 1- and 2-Year Follow-Up Data of 2 Centers
Abstract
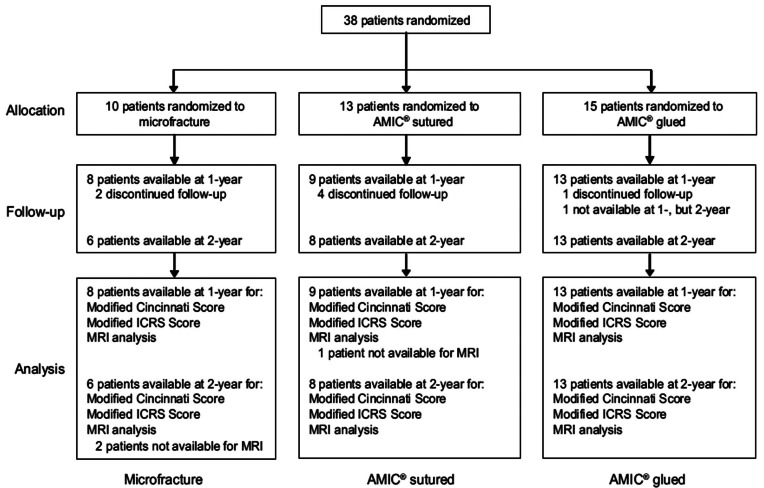
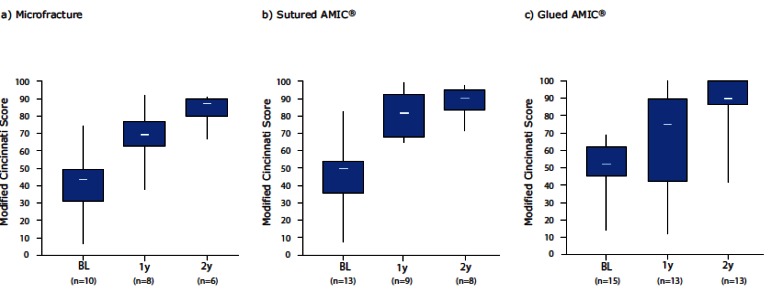
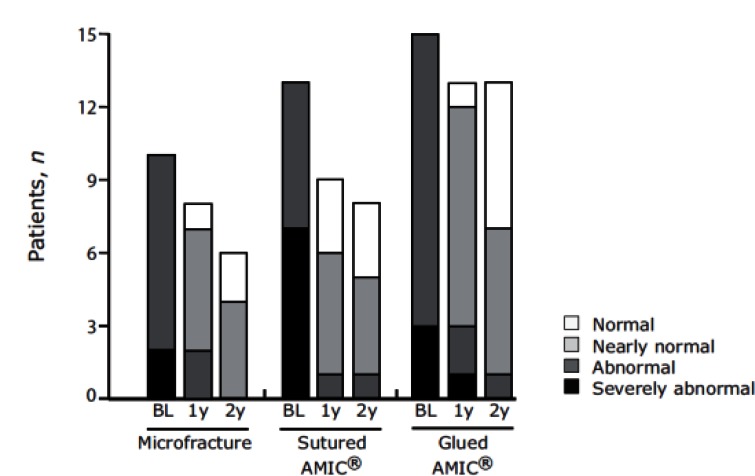
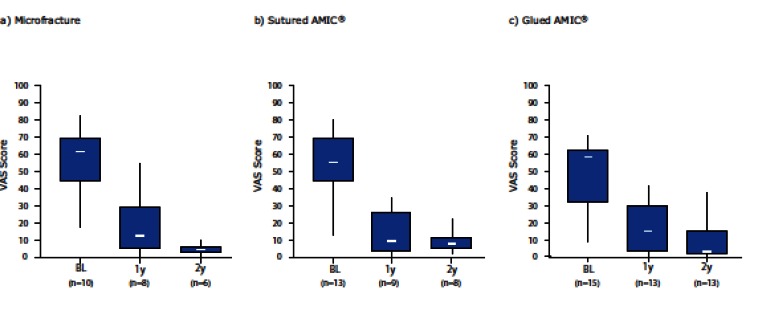
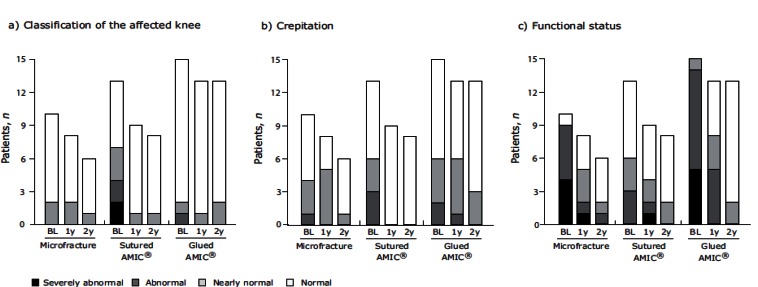
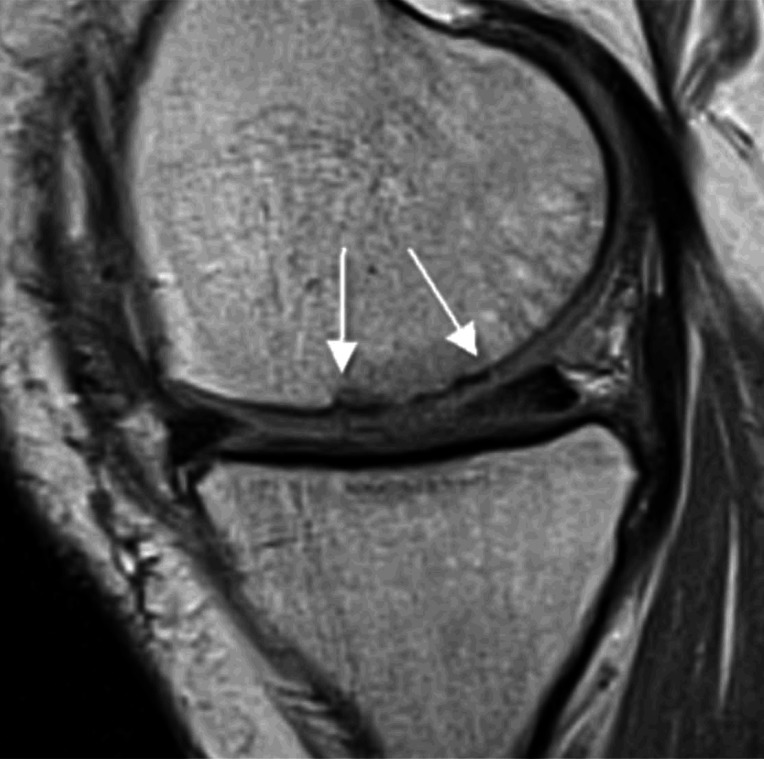
Microfracture (MFx) is currently the recommended option for the treatment of small cartilage defects but is not regarded as suitable for the treatment of defects larger than 2.5 cm(2). To extent its applicability to medium-sized defects MFx has been combined with a collagen type I/III matrix (Chondro-Gide(®)). This technique is called Autologous Matrix-Induced Chondrogenesis (AMIC(®)) and meanwhile a clinically established treatment option for localized full-thickness small- to medium-sized cartilage defects. Despite its more spreading clinical use, clinical data published so far are limited to mainly case report series. In this study, we report the first results of a randomized, controlled trial assessing the efficacy and safety of AMIC(®) versus MFx. Patients enrolled in 2 centers were included in this analysis. 38 patients (aged 21-50 years, mean defect size 3.4 cm(2)) were randomized and treated either with MFx, with sutured AMIC(®) or glued AMIC(®). Clinical outcomes (modified Cincinnati and ICRS score) could be assessed in 30 patients at 1-year and 27 patients at 2-years post-operation. Improvements in both scores were seen at 1-and 2-years post-operation, irrespective of the technique used. MRI assessment revealed a satisfactory and homogenous defect filling in the majority of patients. No treatment-related adverse events were reported. This interim analysis confirms the mid-term results for AMIC(®) reported in literature. It demonstrates clearly that clinical outcomes at 1-year post-operation are maintained at 2-years. Therefore we consider enhancing MFx with Chondro-Gide (®) is a valid and safe cartilage repair option for small- to medium-sized cartilage defects of the knee.
Keywords: Articular cartilage; Autologous matrix-induced chondrogenesis (AMIC®); Chondro-Gide®; knee surgery.; microfracture.
Figures
References
-
- Gelber AC, Hochberg MC, Mead LA, Wang NY, Wigley FM, Klag MJ. Joint injury in young adults and risk for subsequent knee and hip osteoarthritis. Ann Intern Med. 2000;133(5):321–8. - PubMed
-
- Steinwachs MR, Guggi T, Kreuz PC. Marrow stimulation techniques. Injury. 2008;39 (Suppl 1 ):S26–31. - PubMed
-
- Steadman JR, Rodkey WG, Briggs KK, Rodrigo JJ. The microfracture technic in the management of complete cartilage defects in the knee joint. Orthopade. 1999;28(1):26–32. - PubMed
-
- Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture surgical technique and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001;(391 Suppl ):S362–9. - PubMed
-
- Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG. Outcomes of microfracture for traumatic chondral defects of the knee: average 11-year follow-up. Arthroscopy. 2003;19(5):477–84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical