

The consequences of poor communication during transitions from hospital to skilled nursing facility: a qualitative study
- PMID: 23731003
- PMCID: PMC3714367
- DOI: 10.1111/jgs.12328
The consequences of poor communication during transitions from hospital to skilled nursing facility: a qualitative study
Abstract
Objectives: To examine how skilled nursing facility (SNF) nurses transition the care of individuals admitted from hospitals, the barriers they experience, and the outcomes associated with variation in the quality of transitions.
Design: Qualitative study using grounded dimensional analysis, focus groups, and in-depth interviews.
Setting: Five Wisconsin SNFs.
Participants: Twenty-seven registered nurses.
Measurements: Semistructured questions guided the focus group and individual interviews.
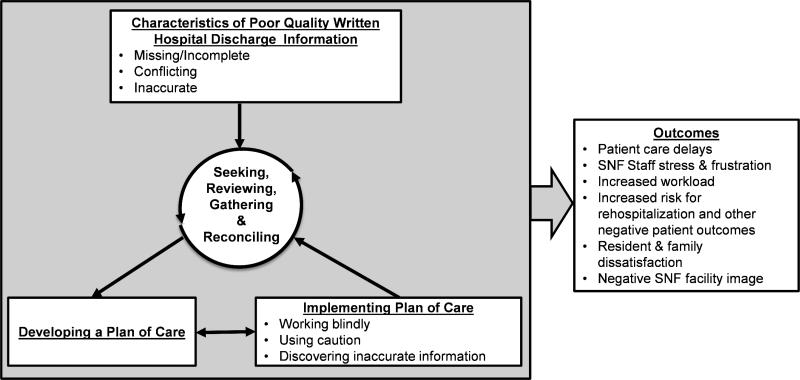
Results: SNF nurses rely heavily on written hospital discharge communication to transition individuals into the SNF effectively. Nurses cited multiple inadequacies of hospital discharge information, including regular problems with medication orders (including the lack of opioid prescriptions for pain), little psychosocial or functional history, and inaccurate information regarding current health status. These communication inadequacies necessitated repeated telephone clarifications, created care delays (including delays in pain control), increased SNF staff stress, frustrated individuals and family members, contributed directly to negative SNF facility image, and increased risk of rehospitalization. SNF nurses identified a specific list of information and components that they need to facilitate a safe, high-quality transition.
Conclusion: Nurses note multiple deficiencies in hospital-to-SNF transitions, with poor quality discharge communication being identified as the major barrier to safe and effective transitions. This information should be used to refine and support the dissemination of evidence-based interventions that support transitions of care, including the Interventions to Reduce Acute Care Transfers program.
Keywords: care transitions; communication; hospital to skilled nursing facility.
© 2013, Copyright the Authors Journal compilation © 2013, The American Geriatrics Society.
Figures
Comment in
-
Re: the consequences of poor communication during transitions from hospital to skilled nursing facility: a qualitative study.J Urol. 2014 May;191(5):1364-5. doi: 10.1016/j.juro.2014.01.060. Epub 2014 Jan 17. J Urol. 2014. PMID: 24745528 No abstract available.
-
Far too easy: opioid diversion during the transition from hospital to nursing home.J Am Geriatr Soc. 2014 Nov;62(11):2229-31. doi: 10.1111/jgs.13084. J Am Geriatr Soc. 2014. PMID: 25413206 Free PMC article. No abstract available.
References
-
- Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. J Am Med Assoc. 2007;297:831–841. - PubMed
-
- Schoenborn NL, Arbaje AI, Eubank KJ, et al. Clinician Roles and Responsibilities During Care Transitions of Older Adults. J Am Geriatr Soc. 2013 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
