

Evaluation of the reliability of clinical staging of T2 N0 esophageal cancer: a review of the Society of Thoracic Surgeons database
- PMID: 23731608
- PMCID: PMC4017898
- DOI: 10.1016/j.athoracsur.2013.03.093
Evaluation of the reliability of clinical staging of T2 N0 esophageal cancer: a review of the Society of Thoracic Surgeons database
Abstract
Background: Clinical staging of esophageal cancer has improved with positron-emission tomography/computed tomography and endoscopic ultrasound imaging. Despite such progress, small single-center studies have questioned the reliability of clinical staging of T2 N0 esophageal cancer. This study broadly examines the adequacy of clinical staging of T2 N0 disease using The Society of Thoracic Surgeons database.
Methods: We retrospectively studied 810 clinical stage T2 N0 patients from 2002 to 2011, with 58 excluded because of incomplete pathologic staging data. Clinical stage, pathologic stage, and preoperative characteristics were recorded. Logistic regression analysis was used to identify factors associated with upstaging at the time of surgical intervention.
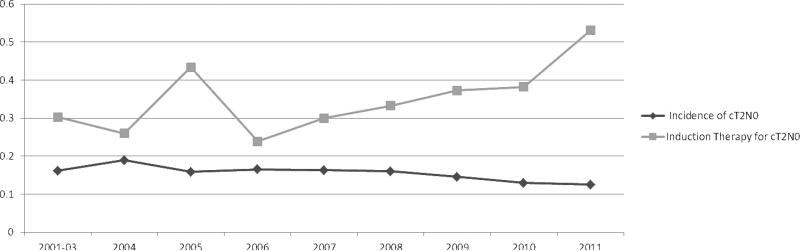
Results: Among 752 clinical stage T2 N0 patients, 270 (35.9%) received induction therapy before the operation. Of 482 patients who went directly to surgical intervention, 132 (27.4%) were confirmed as pathologic T2 N0, 125 (25.9%) were downstaged (ie, T0-1 N0), and 225 (46.7%) were upstaged at the operation (T3-4 N0 or Tany N1-3). Exclusive tumor upstaging (ie, pathologic T3-4 N0) accounted for 41 patients (18.2%), whereas exclusive nodal upstaging (ie, pathological T1-2 N1-3) accounted for 100 (44.5%). Combined tumor and nodal upstaging (ie, pathological T3-4 N1-3) accounted for 84 patients (37.3%). Among patients who received induction therapy, 103 (38.1%) were upstaged vs 225 (46.7%) without induction therapy (p = 0.026). Comparing the induction therapy group and the primary surgical group, postoperative 30-day mortality (3.7% vs 3.7%, p > 0.99) and morbidity (46.3% vs 45%, p = 0.76) were similar.
Conclusions: Despite advances in staging techniques, clinical staging of T2 N0 esophageal cancer remains unreliable. Recognizing T2 N0 as a threshold for induction therapy in esophageal cancer, many surgeons have opted to treat T2 N0 disease with induction therapy, even though one-quarter of these patients will be pathologic T1 N0. Although this study demonstrated similar perioperative morbidity and mortality with and without induction therapy, further study is needed to examine the effect of upstaging on long-term survival.
Keywords: 7; ASA; American Society of Anesthesiologists; CI; CROSS; CT; Chemoradiotherapy for Oesophageal Cancer Followed by Surgery Study; EMR; EUS; FN; FNA; FP; G1; G2; G3; G4; GTSDB; General Thoracic Surgery Database; Gx; NPV; Negative predictive value; OR; PET; PPV; Pathologic staging; Positron emission tomography; SD; STS; Society of Thoracic Surgeons; TN; TP; True positive; c; clinical staging; computed tomography; confidence interval; esophageal mucosal resection; esophageal ultrasound; false negative; false positive; fine needle aspiration; grade moderately differentiated; grade poorly differentiated; grade undetermined; grade undifferentiated; grade well differentiated; odds ratio; p; positive predictive value; standard deviation; true negative.
Copyright © 2013 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Endoscopic ultrasound for early stage esophageal adenocarcinoma: implications for staging and survival.Ann Thorac Surg. 2011 May;91(5):1509-15; discussion 1515-6. doi: 10.1016/j.athoracsur.2011.01.063. Epub 2011 Mar 24. Ann Thorac Surg. 2011. PMID: 21435632
-
Implementation of Staging Guidelines in Early Esophageal Cancer: A Study of the Society of Thoracic Surgeons General Thoracic Surgery Database.Ann Surg. 2023 Oct 1;278(4):e754-e759. doi: 10.1097/SLA.0000000000005837. Epub 2023 Mar 13. Ann Surg. 2023. PMID: 36912032 Free PMC article.
-
Clinical T2N0 Esophageal Cancer: Identifying Pretreatment Characteristics Associated With Pathologic Upstaging and the Potential Role for Induction Therapy.Ann Thorac Surg. 2016 Jun;101(6):2102-11. doi: 10.1016/j.athoracsur.2016.01.033. Epub 2016 Apr 12. Ann Thorac Surg. 2016. PMID: 27083246 Free PMC article.
-
Neoadjuvant chemoradiation therapy is beneficial for clinical stage T2 N0 esophageal cancer patients due to inaccurate preoperative staging.Ann Thorac Surg. 2012 Feb;93(2):429-35; discussion 436-7. doi: 10.1016/j.athoracsur.2011.10.061. Ann Thorac Surg. 2012. PMID: 22269708 Free PMC article. Review.
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
Cited by
-
Collaborative multidisciplinary management and expertise of cT2-3 locally advanced operable esophageal squamous cell carcinoma: a report of two cases.J Thorac Dis. 2023 Nov 30;15(11):6362-6372. doi: 10.21037/jtd-23-1277. Epub 2023 Nov 21. J Thorac Dis. 2023. PMID: 38090303 Free PMC article.
-
Clinical staging to differentiate T2 and T3 esophageal squamous cell carcinomas-essential details or just noise?J Thorac Dis. 2024 Nov 30;16(11):7230-7232. doi: 10.21037/jtd-24-491. Epub 2024 Nov 29. J Thorac Dis. 2024. PMID: 39678881 Free PMC article. No abstract available.
-
Prognostic relevance of lymph node regression on survival in esophageal cancer: a systematic review and meta-analysis.Dis Esophagus. 2022 Jan 7;35(1):doab021. doi: 10.1093/dote/doab021. Dis Esophagus. 2022. PMID: 33893494 Free PMC article.
-
cT2N0 esophageal adenocarcinoma: predictors of lymph nodal involvement and clinical significance.J Thorac Dis. 2019 Mar;11(Suppl 3):S453-S456. doi: 10.21037/jtd.2018.11.24. J Thorac Dis. 2019. PMID: 30997246 Free PMC article. No abstract available.
-
Neoadjuvant treatment of locally advanced esophageal and junctional cancer: the evidence-base, current key questions and clinical trials.J Thorac Dis. 2017 Jul;9(Suppl 8):S697-S704. doi: 10.21037/jtd.2017.03.159. J Thorac Dis. 2017. PMID: 28815065 Free PMC article. Review.
References
-
- Urschel JD, Vasan H, Blewett CJ. A meta-analysis of randomized controlled trials that compared neoadjuvant chemotherapy and surgery to surgery alone for resectable esophageal cancer. Am J Surg. 2002;183(3):274–9. - PubMed
-
- Graham AJ, et al. Defining the optimal treatment of locally advanced esophageal cancer: a systematic review and decision analysis. Ann Thorac Surg. 2007;83(4):1257–64. - PubMed
-
- van Hagen P, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–84. - PubMed
-
- Malthaner R, Wong RK, Spithoff K. Preoperative or postoperative therapy for resectable oesophageal cancer: an updated practice guideline. Clin Oncol (R Coll Radiol) 2010;22(4):250–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
