

Managing patients with stable respiratory disease planning air travel: a primary care summary of the British Thoracic Society recommendations
- PMID: 23732637
- PMCID: PMC6442792
- DOI: 10.4104/pcrj.2013.00046
Managing patients with stable respiratory disease planning air travel: a primary care summary of the British Thoracic Society recommendations
Abstract
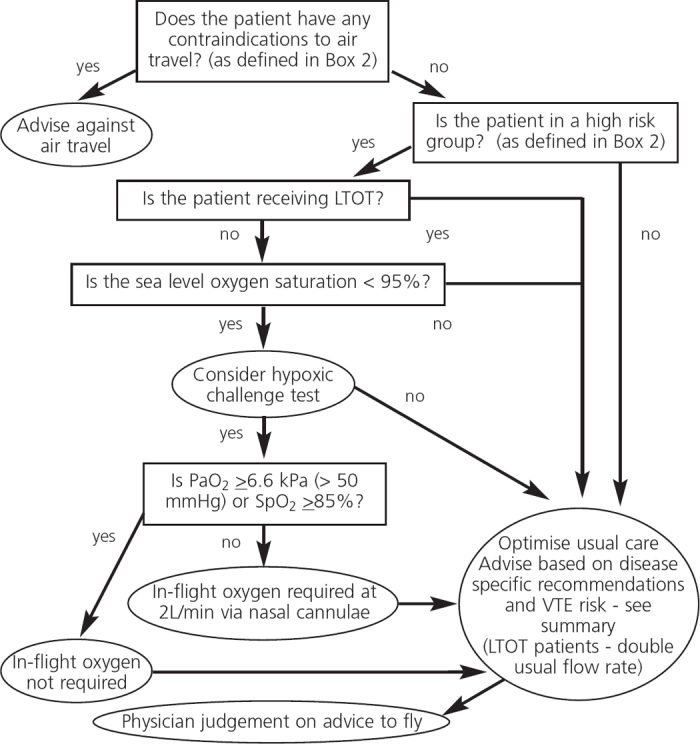
Air travel poses medical challenges to passengers with respiratory disease, principally because of exposure to a hypobaric environment. In 2002 the British Thoracic Society published recommendations for adults and children with respiratory disease planning air travel, with a web update in 2004. New full recommendations and a summary were published in 2011, containing key recommendations for the assessment of high-risk patients and identification of those likely to require in-flight supplemental oxygen. This paper highlights the aspects of particular relevance to primary care practitioners with the following key points: (1) At cabin altitudes of 8000 feet (the usual upper limit of in-flight cabin pressure, equivalent to 0.75 atmospheres) the partial pressure of oxygen falls to the equivalent of breathing 15.1% oxygen at sea level. Arterial oxygen tension falls in all passengers; in patients with respiratory disease, altitude may worsen preexisting hypoxaemia. (2) Altitude exposure also influences the volume of any air in cavities, where pressure x volume remain constant (Boyle's law), so that a pneumothorax or closed lung bulla will expand and may cause respiratory distress. Similarly, barotrauma may affect the middle ear or sinuses if these cavities fail to equilibrate. (3) Patients with respiratory disease require clinical assessment and advice before air travel to: (a) optimise usual care; (b) consider contraindications to travel and possible need for in-flight oxygen; (c) consider the need for secondary care referral for further assessment; (d) discuss the risk of venous thromboembolism; and (e) discuss forward planning for the journey.
Conflict of interest statement
The authors declare that they have no conflicts of interest in relation to this article. MT is an Associate editor of the
Figures
References
-
- Akero A, Christensen CC, Edvardsen A, Ryg M, Skjonsberg OH. Pulse oximetry in the preflight evaluation of patients with chronic obstructive pulmonary disease. Aviat Space Environ Med 2008;79(5):518–24. http://dx.doi.org/10.3357/ASEM.2120.2008 - PubMed
-
- Christensen CC, Ryg M, Refvem OK, Skjonsberg OH. Development of severe hypoxaemia in chronic obstructive pulmonary disease patients at 2,438 m (8,000 ft) altitude. Eur Respir J 2000;15(4):635–9. http://dx.doi.org/10.1183/09031936.00.15463500 - PubMed
-
- Coker RK, Shiner RJ, Partridge MR. Is air travel safe for those with lung disease? Eur Respir J 2007;30(6):1057–63. http://dx.doi.org/10.1183/09031936.00024707 - PubMed
-
- Robson AG, Hartung TK, Innes JA. Laboratory assessment of fitness to fly in patients with lung disease: a practical approach. Eur Respir J 2000;16(2):214–19. http://dx.doi.org/10.1034/j.1399-3003.2000.16b06.x - PubMed
-
- Schwartz JS, Bencowitz HZ, Moser KM. Air travel hypoxemia with chronic obstructive pulmonary disease. Ann Intern Med 1984;100(4):473–7. http://dx.doi.org/10.7326/0003-4819-100-4-473 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources