

Atrial selectivity of antiarrhythmic drugs
- PMID: 23732646
- PMCID: PMC3779104
- DOI: 10.1113/jphysiol.2013.256115
Atrial selectivity of antiarrhythmic drugs
Abstract
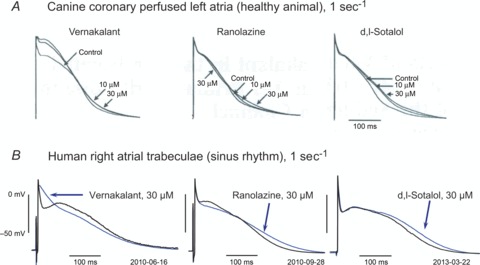
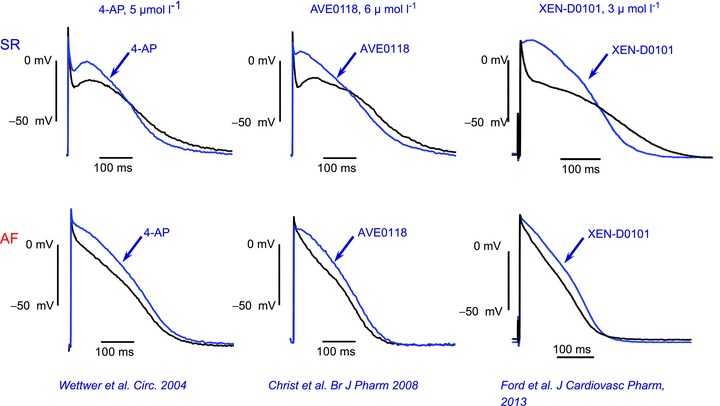
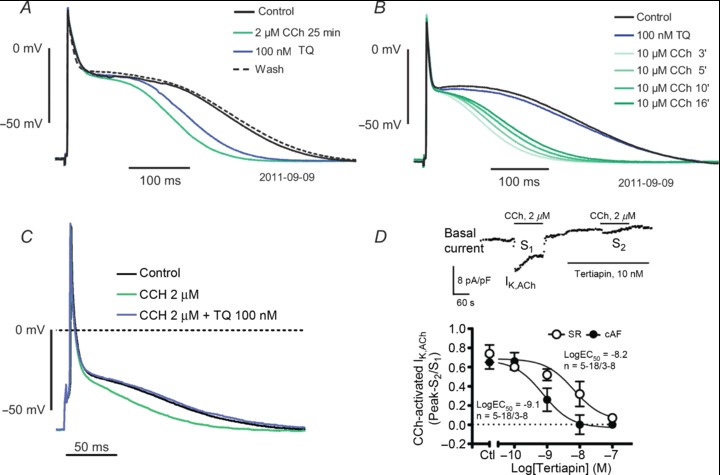
New antiarrhythmic drugs for treatment of atrial fibrillation should ideally be atrial selective in order to avoid pro-arrhythmic effects in the ventricles. Currently recognized atrial selective targets include atrial Nav1.5 channels, Kv1.5 channels and constitutively active Kir3.1/3.4 channels, each of which confers atrial selectivity by different mechanisms. Na(+) channel blockers with potential- and frequency-dependent action preferentially suppress atrial fibrillation because of the high excitation rate and less negative atrial resting potential, which promote drug binding in atria. Kv1.5 channels are truly atrial selective because they do not conduct repolarizing current IKur in ventricles. Constitutively active IK,ACh is predominantly observed in remodelled atria from patients in permanent atrial fibrillation (AF). A lot of effort has been invested to detect compounds which will selectively block Kir3.1/Kir3.4 in their remodelled constitutively active form. Novel drugs which have been and are being developed aim at atrial-selective targets. Vernakalant and ranolazine which mainly block atrial Na(+) channels are clinically effective. Newly designed selective IKur blockers and IK,ACh blockers are effective in animal models; however, clinical benefit in converting AF into sinus rhythm (SR) or reducing AF burden remains to be demonstrated. In conclusion, atrial-selective antiarrhythmic agents have a lot of potential, but a long way to go.
Figures
References
-
- Allessie M, Ausma J, Schotten U. Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc Res. 2002;54:230–246. - PubMed
-
- Aonuma S, Kohama Y, Akai K, Komiyama Y, Nakajima S, Wakabayashi M, Makino T. Studies on heart. XIX. Isolation of an atrial peptide that improves the rhythmicity of cultured myocardial cell clusters. Chem Pharm Bull (Tokyo) 1980;28:3332–3339. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials