

Diagnostic value of sTREM-1 in bronchoalveolar lavage fluid in ICU patients with bacterial lung infections: a bivariate meta-analysis
- PMID: 23734253
- PMCID: PMC3667178
- DOI: 10.1371/journal.pone.0065436
Diagnostic value of sTREM-1 in bronchoalveolar lavage fluid in ICU patients with bacterial lung infections: a bivariate meta-analysis
Abstract
Background: The serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) is a useful biomarker in differentiating bacterial infections from others. However, the diagnostic value of sTREM-1 in bronchoalveolar lavage fluid (BALF) in lung infections has not been well established. We performed a meta-analysis to assess the accuracy of sTREM-1 in BALF for diagnosis of bacterial lung infections in intensive care unit (ICU) patients.
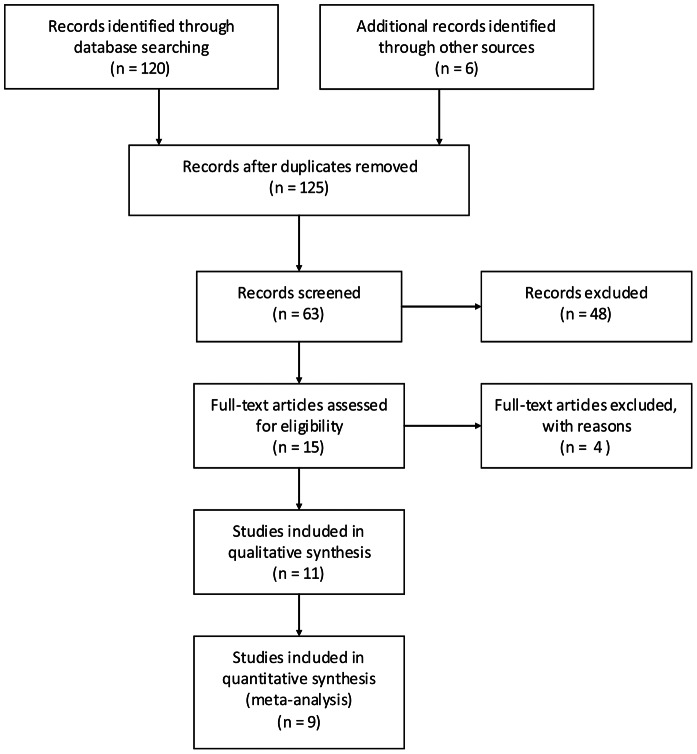
Methods: We searched PUBMED, EMBASE and Web of Knowledge (from January 1966 to October 2012) databases for relevant studies that reported diagnostic accuracy data of BALF sTREM-1 in the diagnosis of bacterial lung infections in ICU patients. Pooled sensitivity, specificity, and positive and negative likelihood ratios were calculated by a bivariate regression analysis. Measures of accuracy and Q point value (Q*) were calculated using summary receiver operating characteristic (SROC) curve. The potential between-studies heterogeneity was explored by subgroup analysis.
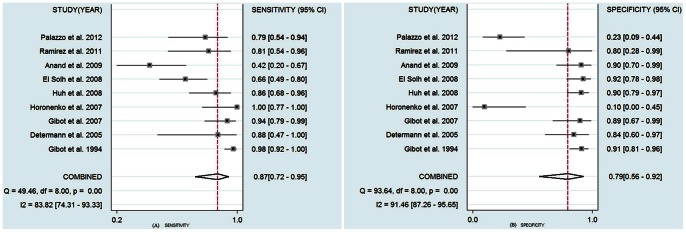
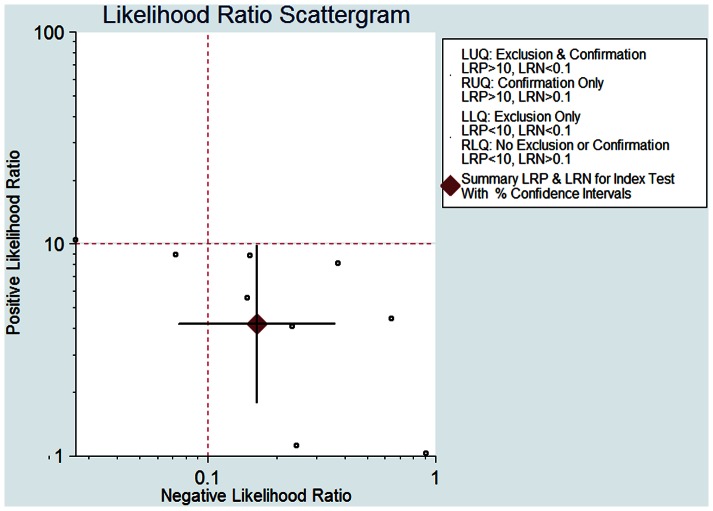
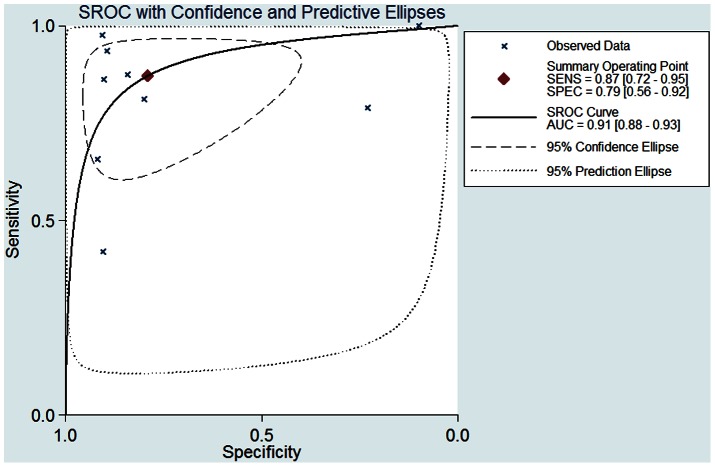
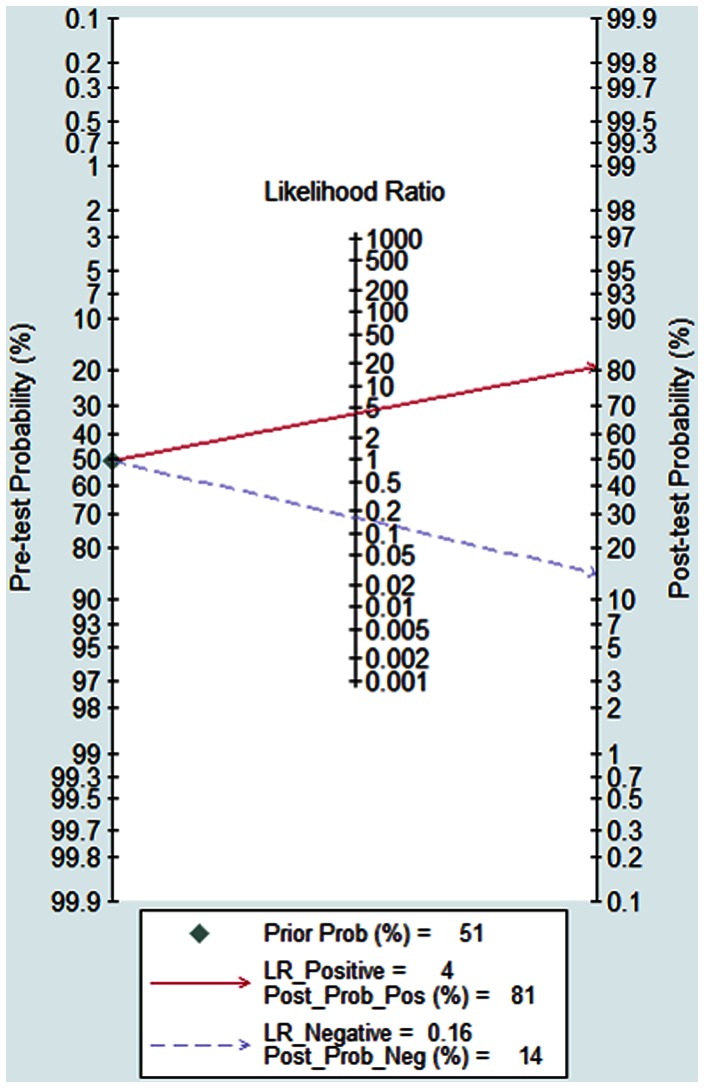
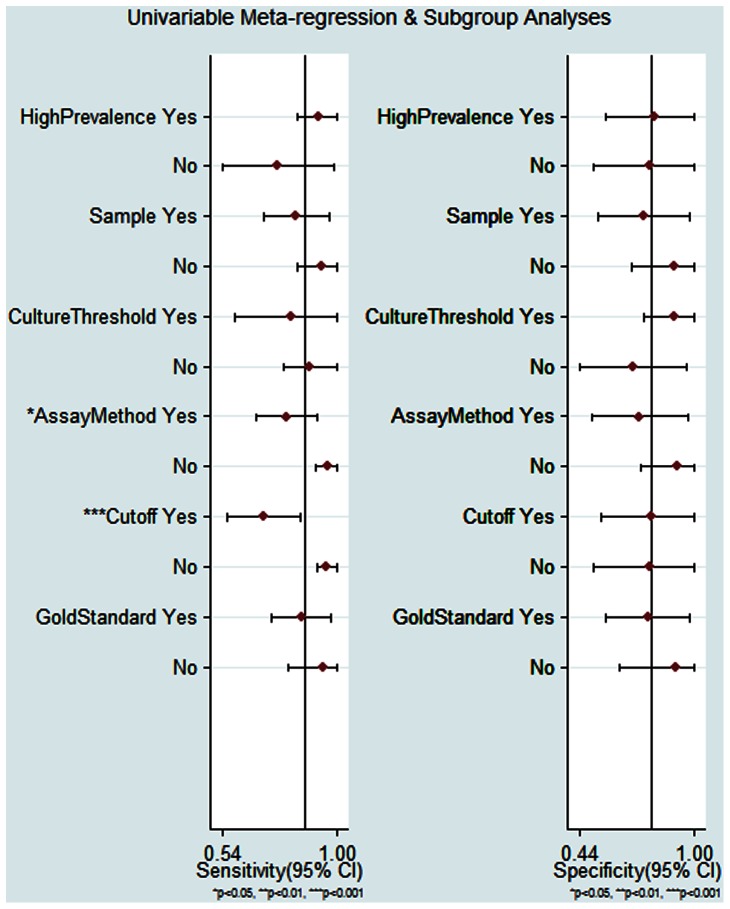
Results: Nine studies were included in the present meta-analysis. Overall, the prevalence was 50.6%; the sensitivity was 0.87 (95% confidence interval (CI), 0.72-0.95); the specificity was 0.79 (95% CI, 0.56-0.92); the positive likelihood ratio (PLR) was 4.18 (95% CI, 1.78-9.86); the negative likelihood ratio (NLR) was 0.16 (95% CI, 0.07-0.36), and the diagnostic odds ratio (DOR) was 25.60 (95% CI, 7.28-89.93). The area under the SROC curve was 0.91 (95% CI, 0.88-0.93), with a Q* of 0.83. Subgroup analysis showed that the assay method and cutoff value influenced the diagnostic accuracy of sTREM-1.
Conclusions: BALF sTREM-1 is a useful biomarker of bacterial lung infections in ICU patients. Further studies are needed to confirm the optimized cutoff value.
Conflict of interest statement
Figures
References
-
- Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, et al. (1995) The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA 274: 639–644. - PubMed
-
- Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH (2002) Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest 122: 262–268. - PubMed
-
- Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret GY (2006) Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis. Crit Care Med 34: 1996–2003. - PubMed
-
- Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, et al. (2004) Soluble triggering receptor expressed on myeloid cells and the diagnosis of pneumonia. N Engl J Med 350: 451–458. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
