

A case report of syndrome of inappropriate antidiuretic hormone secretion with Castleman's disease and lymphoma
- PMID: 23734852
- PMCID: PMC3679987
- DOI: 10.1186/1472-6823-13-19
A case report of syndrome of inappropriate antidiuretic hormone secretion with Castleman's disease and lymphoma
Abstract
Background: Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is a common cause of hyponatremia in hospitalized patients and is often described in patients with small-cell carcinoma of the lung. In this report, we described both Castleman's disease and lymphoma coexisting in one patient with SIADH.
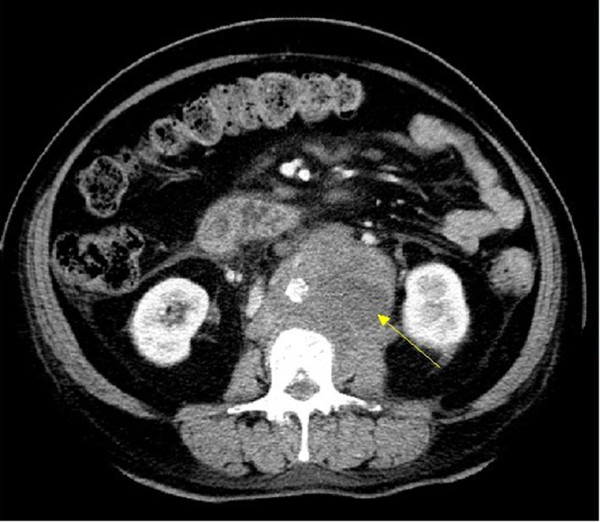
Case presentation: A 70-year-old Chinese woman with a history of diabetes mellitus and insulin therapy had severe hyponatremia and gastrointestinal symptoms. Through a series of examinations, common causes such as pulmonary carcinoma were excluded. An abdominal mass was detected by computed tomography. Although the peripheral lymph node biopsy showed the pathological result as Castleman's disease, the pathology of the abdominal lymph node revealed diffuse large B-cell lymphoma. After chemotherapy, the hyponatremia was treated during a period of follow-up.
Conclusion: This patient presented with the rare clinical condition of inappropriate antidiuretic hormone secretion alongside Castleman's disease and lymphoma. Asymptomatic hyponatremia may persist for some time suggesting that clinical physicians should pay attention to the mild cases of hyponatremia. We also hypothesized that Castleman's disease is a condition of pre-lymphoma with both having the ability to cause SIADH. The possibility of lymphoma as well as Castleman's disease triggering the development of SIADH should also be taken into consideration for conducting recurrent biopsies.
Figures


References
-
- Upadhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia. Am J Med. 2006;119(7 Suppl 1):S30–S35. - PubMed
-
- Schwartz WB, Bennett W, Curelop S, Bartter FC. A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. J Am Soc Nephrol. 1957;12(12):2860–2870. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
