

Managing psychiatric comorbidity within versus outside of methadone treatment settings: a randomized and controlled evaluation
- PMID: 23734943
- PMCID: PMC3833440
- DOI: 10.1111/add.12269
Managing psychiatric comorbidity within versus outside of methadone treatment settings: a randomized and controlled evaluation
Abstract
Background and aims: Integrating psychiatric services within substance abuse treatment settings is a promising service delivery model, but has not been evaluated using random assignment to psychiatric treatment setting and controlled delivery of psychiatric care. This study evaluates the efficacy of on-site and integrated psychiatric service delivery in an opioid-agonist treatment program on psychiatric and substance use outcomes.
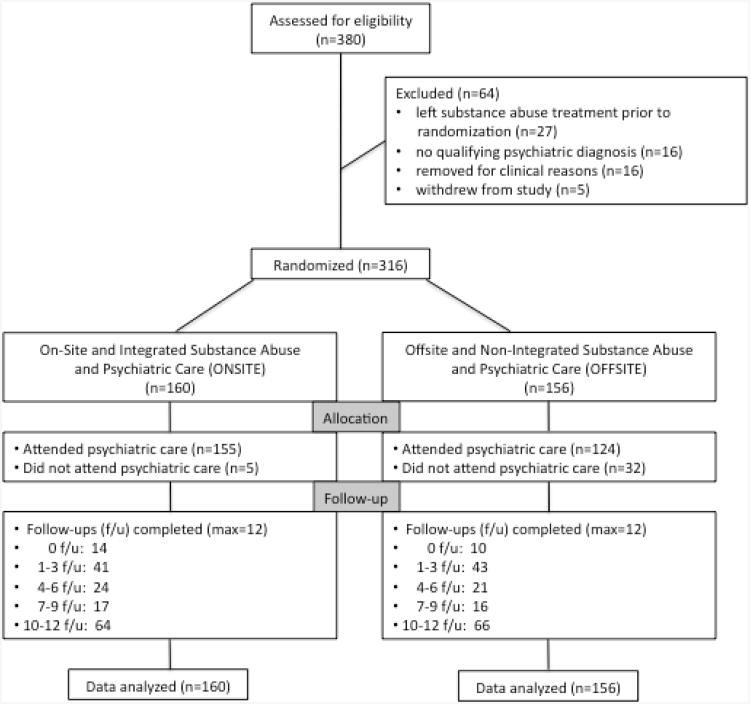
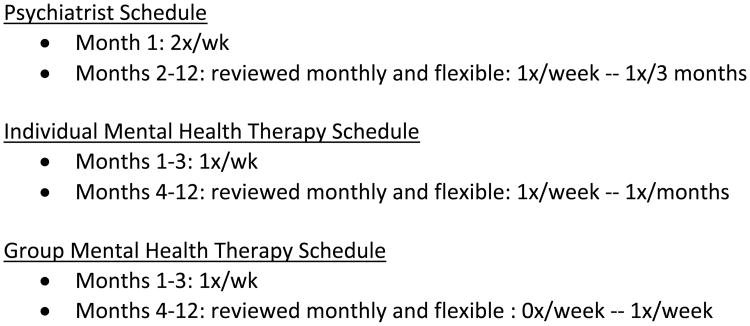
Design: Participants at the Addiction Treatment Services (ATS) were assigned randomly to receive on-site and integrated substance abuse and psychiatric care (on-site: n = 160) versus off-site and non-integrated substance abuse and psychiatric care (off-site: n = 156), and observed for 1 year. On-site participants received all psychiatric care within the substance abuse program by the same group of treatment providers. The same type and schedule of psychiatric services were available to off-site participants at a community psychiatry program.
Setting: All participants received routine methadone maintenance at the ATS program in Baltimore, Maryland, USA.
Participants: Participants were opioid-dependent men and women with at least one comorbid psychiatric disorder, as assessed by the Structured Clinical Interview for DSM-IV and confirmed by expert clinical reappraisal.
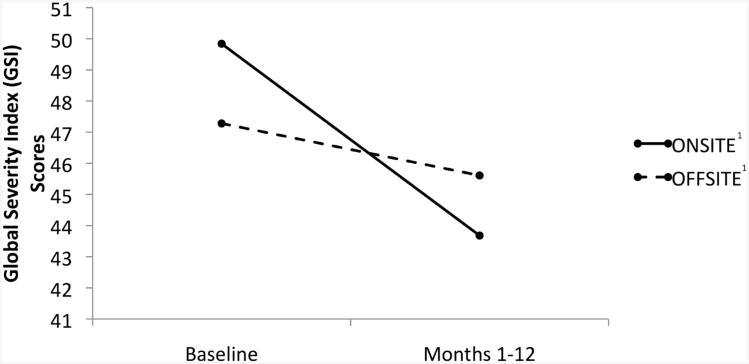
Measurements: Outcomes included psychiatric service utilization and retention, Hopkins Symptom Checklist Global Severity Index (GSI) change scores and urinalysis test results.
Findings: On-site participants were more likely to initiate psychiatric care 96.9 to 79.5%; P < 0.001), remain in treatment longer (195.9 versus 101.9 days; P < 0.001), attend more psychiatrist appointments (12.9 versus 2.7; P < 0.001) and have greater reductions in GSI scores (4.2 versus 1.7; P = 0.003) than off-site participants; no differences were observed for drug use.
Conclusions: On-site and integrated psychiatric and substance misuse services in a methadone treatment setting might improve psychiatric outcomes compared with off-site and non-integrated substance misuse and psychiatric care. However, this might not translate into improved substance misuse outcomes.
Keywords: Drug use; integrated care; methadone maintenance; psychiatric care; psychiatric comorbidity; treatment response.
© 2013 Society for the Study of Addiction.
Figures
Comment in
-
Commentary on Brooner et al. (2013): one-stop shopping--what sells and what doesn't.Addiction. 2013 Nov;108(11):1952-3. doi: 10.1111/add.12340. Addiction. 2013. PMID: 24118760 No abstract available.
References
-
- McLellan AT, Lewis DC, O'Brien CP, Kleber HD. Drug dependence, a chronic medical illness: Implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284:1689–1695. - PubMed
-
- Brooner RK, King VL, Kidorf M, Schmidt CW, Bigelow GE. Psychiatric and substance use comorbidity among treatment-seeking opioid abusers. Arch Gen Psychiatry. 1997;1997;54:71–80. - PubMed
-
- McGovern MP, Xie H, Segal SR, Siembab L, Drake RE. Addiction treatment services and co-occurring disorders. J Subst Abuse Treat. 2006;31:267–275. - PubMed
-
- Bohnert AS, Ilgen MA, Ignacio RV, McCarthy JF, Valenstein M, Blow FC. Risk of death from accidental overdose associated with psychiatric and substance use disorders. Am J Psychiatry. 2012;169:64–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
