

Comorbid diabetes and COPD: impact of corticosteroid use on diabetes complications
- PMID: 23735725
- PMCID: PMC3781532
- DOI: 10.2337/dc12-2197
Comorbid diabetes and COPD: impact of corticosteroid use on diabetes complications
Abstract
Objective: To identify if there is a dose-dependent risk of diabetes complications in patients treated with corticosteroids who have both diabetes and chronic obstructive pulmonary disorder (COPD).
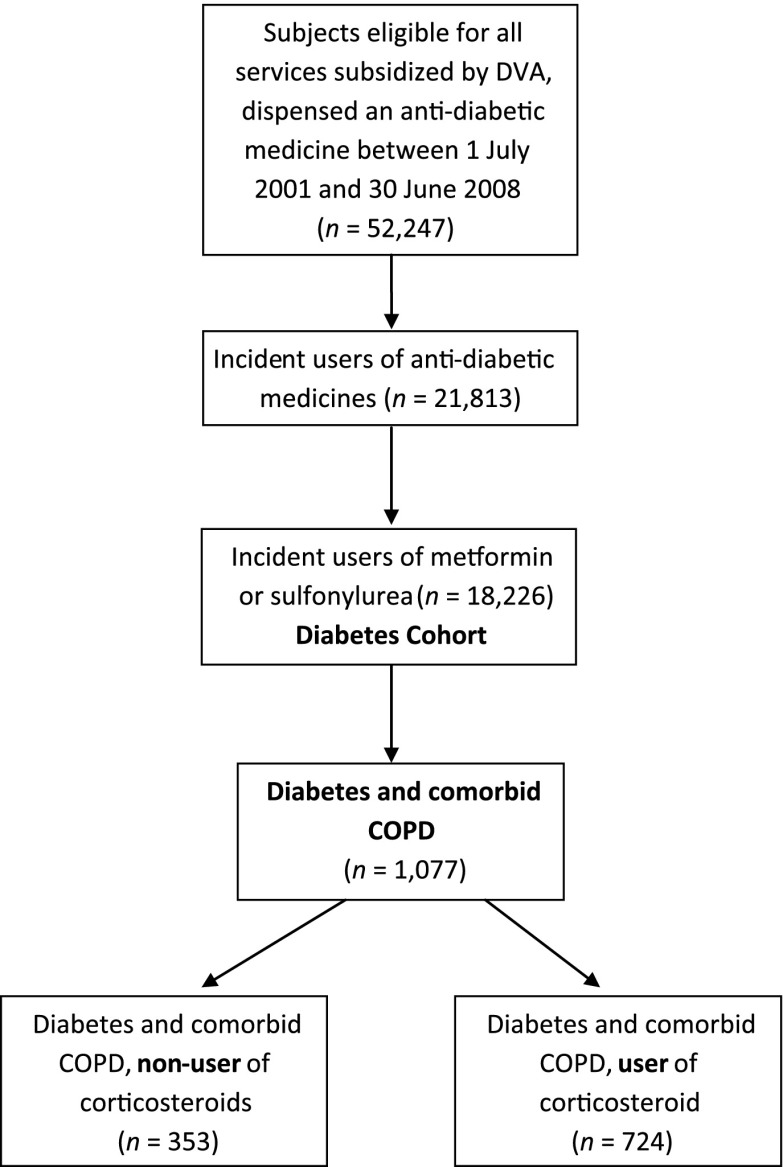
Research design and methods: A retrospective study of administrative claims data from the Australian Government Department of Veterans' Affairs, from 1 July 2001 to 30 June 2008, of diabetes patients newly initiated on metformin or sulfonylurea. COPD was identified by dispensings of tiotropium or ipratropium in the 6 months preceding study entry. Total corticosteroid use (inhaled and systemic) in the 12 months after study entry was determined. The outcome was time to hospitalization for a diabetes-related complication. Competing risks and Cox proportional hazard regression analyses were conducted with adjustment for a number of covariates.
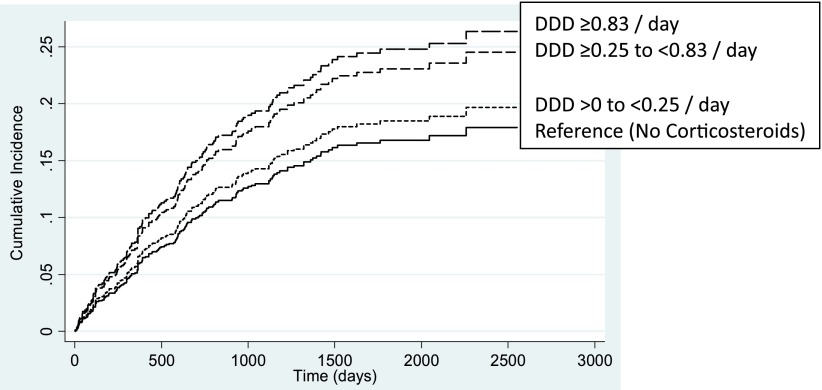
Results: A total of 18,226 subjects with diabetes were identified, of which 5.9% had COPD. Of those with COPD, 67.2% were dispensed corticosteroids in the 12 months from study entry. Stratification by dose of corticosteroids demonstrated a 94% increased likelihood of hospitalization for a diabetes complication for those who received a total defined daily dose (DDD) of corticosteroids≥0.83/day (subhazard ratio 1.94 [95% CI 1.14-3.28], P=0.014), by comparison with those who did not receive a corticosteroid. Lower doses of corticosteroid (<0.83 DDD/day) were not associated with an increased risk of diabetes-related hospitalization.
Conclusions: In patients with diabetes and COPD, an increased risk of diabetes-related hospitalizations was only evident with use of high doses of corticosteroids. This highlights the need for constant revision of corticosteroid dose in those with diabetes and COPD, to ensure that the minimally effective dose is used, together with review of appropriate response to therapy.
Figures
References
-
- Caughey GE, Roughead EE, Vitry AI, McDermott RA, Shakib S, Gilbert AL. Comorbidity in the elderly with diabetes: identification of areas of potential treatment conflicts. Diabetes Res Clin Pract 2010;87:385–393 - PubMed
-
- Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care 2006;29:725–731 - PubMed
-
- Rabe KF, Wedzicha JA. Controversies in treatment of chronic obstructive pulmonary disease. Lancet 2011;378:1038–1047 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
