

Exercise training reduces peripheral arterial stiffness and myocardial oxygen demand in young prehypertensive subjects
- PMID: 23736111
- PMCID: PMC3741227
- DOI: 10.1093/ajh/hpt080
Exercise training reduces peripheral arterial stiffness and myocardial oxygen demand in young prehypertensive subjects
Abstract
Background: Large artery stiffness is a major risk factor for the development of hypertension and cardiovascular disease. Persistent prehypertension accelerates the progression of arterial stiffness.
Methods: Forty-three unmedicated prehypertensive (systolic blood pressure (SBP) = 120-139 mm Hg or diastolic blood pressure (DBP) = 80-89 mm Hg) men and women and 15 normotensive time-matched control subjects (NMTCs; n = 15) aged 18-35 years of age met screening requirements and participated in the study. Prehypertensive subjects were randomly assigned to a resistance exercise training (PHRT; n = 15), endurance exercise training (PHET; n = 13) or time-control group (PHTC; n = 15). Treatment groups performed exercise training 3 days per week for 8 weeks. Pulse wave analysis, pulse wave velocity (PWV), and central and peripheral blood pressures were evaluated before and after exercise intervention or time-matched control.
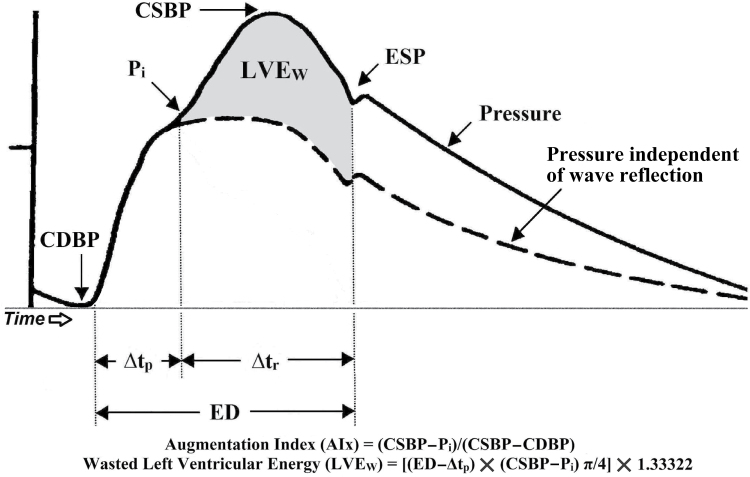
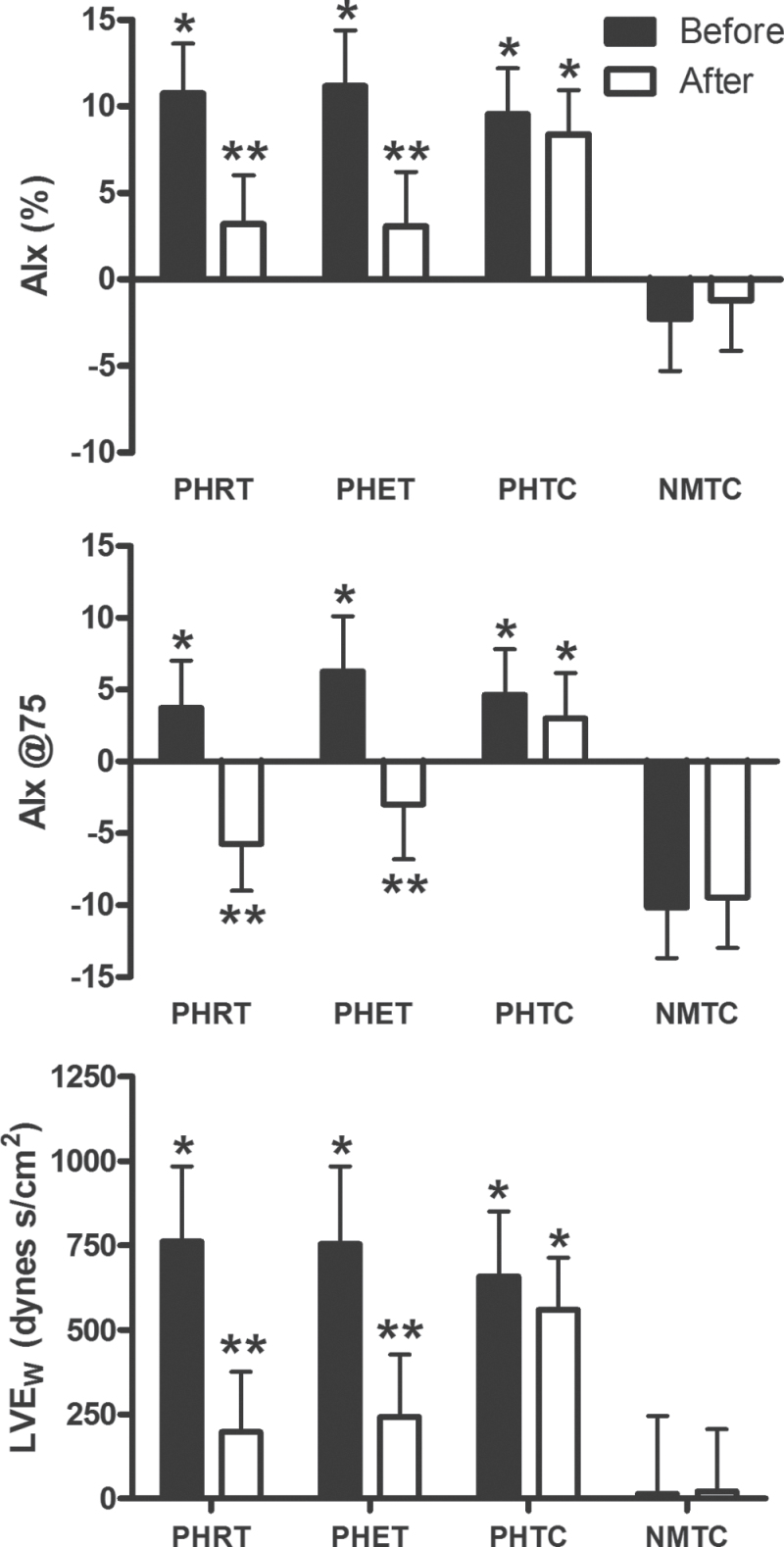
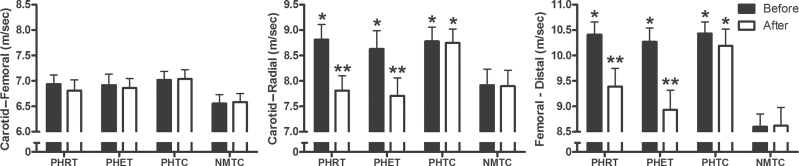
Results: PHRT and PHET reduced resting SBP by 9.6±3.6mm Hg and 11.9±3.4mm Hg, respectively, and DBP by 8.0±5.1mm Hg and 7.2±3.4mm Hg, respectively (P < 0.05). PHRT and PHET decreased augmentation index (AIx) by 7.5% ± 2.8% and 8.1% ± 3.2% (P < 0.05), AIx@75 by 8.0% ± 3.2% and 9.2% ± 3.8% (P < 0.05), and left ventricular wasted pressure energy, an index of extra left ventricular myocardial oxygen requirement due to early systolic wave reflection, by 573±161 dynes s/cm(2) and 612±167 dynes s/cm(2) (P < 0.05), respectively. PHRT and PHET reduced carotid-radial PWV by 1.02±0.32 m/sec and 0.92±0.36 m/sec (P < 0.05) and femoral-distal PWV by 1.04±0.31 m/sec and 1.34±0.33 m/sec (P < 0.05), respectively. No significant changes were observed in the time-control groups.
Conclusions: This study suggests that both resistance and endurance exercise alone effectively reduce peripheral arterial stiffness, central blood pressures, augmentation index, and myocardial oxygen demand in young prehypertensive subjects.
Keywords: arterial stiffness; augmentation index; blood pressure; exercise; hypertension; left ventricular wasted pressure energy; prehypertension..
Figures
References
-
- Ferreira I, van de Laar RJ, Prins MH, Twisk JW, Stehouwer CD. Carotid stiffness in young adults: a life-course analysis of its early determinants: the Amsterdam Growth and Health Longitudinal Study. Hypertension 2012; 59:54–61 - PubMed
-
- Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001; 37:1236–1241 - PubMed
-
- Lakatta EG. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: part III: cellular and molecular clues to heart and arterial aging. Circulation 2003; 107:490–497 - PubMed
-
- Nosaka T, Tanaka H, Watanabe I, Sato M, Matsuda M. Influence of regular exercise on age-related changes in arterial elasticity: mechanistic insights from wall compositions in rat aorta. Can J Appl Physiol 2003; 28:204–212 - PubMed
-
- Gedikli O, Kiris A, Ozturk S, Baltaci D, Karaman K, Durmus I, Baykan M, Celik S. Effects of prehypertension on arterial stiffness and wave reflections. Clin Exp Hypertens 2010; 32:84–89 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
