

Recombinant growth hormone therapy for cystic fibrosis in children and young adults
- PMID: 23737090
- PMCID: PMC4465600
- DOI: 10.1002/14651858.CD008901.pub2
Recombinant growth hormone therapy for cystic fibrosis in children and young adults
Update in
-
Recombinant growth hormone therapy for cystic fibrosis in children and young adults.Cochrane Database Syst Rev. 2015 May 20;(5):CD008901. doi: 10.1002/14651858.CD008901.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2018 Dec 17;12:CD008901. doi: 10.1002/14651858.CD008901.pub4. PMID: 25991406 Updated.
Abstract
Background: Cystic fibrosis is an inherited condition causing disease most noticeably in the lungs, digestive tract and pancreas. People with cystic fibrosis often have malnutrition and growth delay. Adequate nutritional supplementation does not improve growth optimally and hence an anabolic agent, recombinant growth hormone, has been proposed as a potential intervention.
Objectives: To evaluate the effectiveness and safety of recombinant human growth hormone therapy in improving lung function, quality of life and clinical status of children and young adults with cystic fibrosis.
Search methods: We searched the Cochrane Cystic Fibrosis and Genetic Disorders Group's Trials Register comprising references identified from comprehensive electronic database searches and handsearches of relevant journals and abstract books of conference proceedings. Date of latest search: 15 May 2013.We conducted a search of relevant endocrine journals and proceedings of the Endocrinology Society meetings using Scopus and Proceedings First. Date of latest search: 15 March 2012.
Selection criteria: Randomised and quasi-randomised controlled trials of all preparations of recombinant growth hormone compared to either no treatment, or placebo, or each other at any dose (high-dose and low-dose) or route and for any duration, in children or young adults aged up to 25 years diagnosed with cystic fibrosis (by sweat test or genetic testing).
Data collection and analysis: Two authors independently screened papers, extracted trial details and assessed their risk of bias.
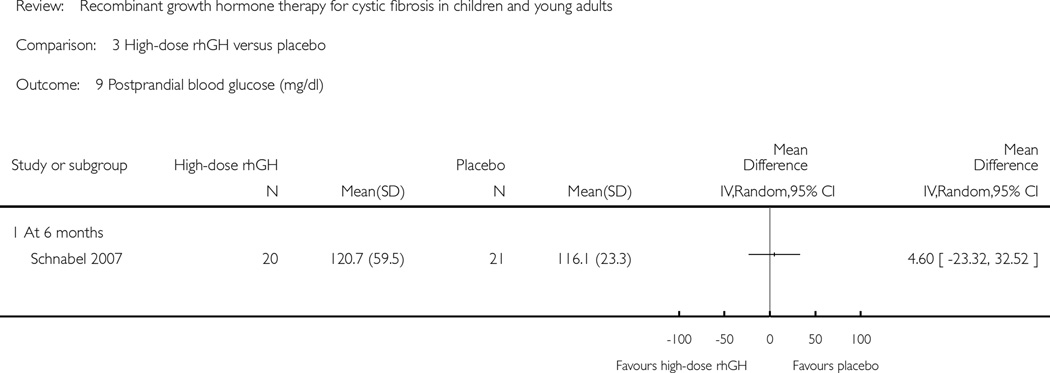
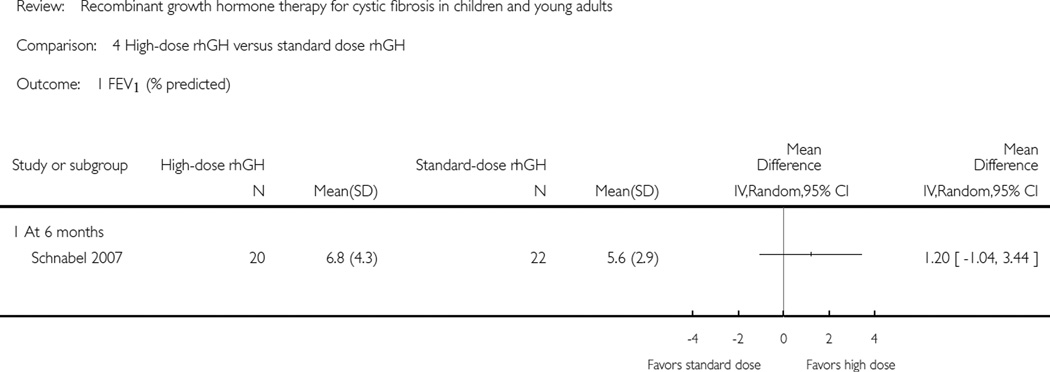
Main results: Four controlled trials were included in this review (with 161 participants in total), each with an unclear risk of bias. Analysis of data obtained from these trials shows improvement in height for all comparisons, but improvements in weight and lean tissue mass were only reported in the comparison of standard dose recombinant growth hormone versus no treatment. There is moderate improvement in one parameter of pulmonary function tests, functional vital capacity (per cent predicted) when comparing standard dose recombinant growth hormone and no treatment. Little evidence was found for improvement in quality of life. An improvement in fasting blood glucose levels was reported when comparing rhGH to placebo only. Exercise capacity improved in participants receiving standard dose recombinant growth hormone versus no treatment, but not for any other comparison. There is insufficient evidence to conclude any changes in hospitalisations, antibiotic use or significant adverse effects.
Authors' conclusions: Recombinant growth hormone therapy is effective in improving the intermediate outcomes in height, weight and lean tissue mass when compared with no treatment. One measure of pulmonary function test showed moderate improvement. No significant changes in quality of life, clinical status or side-effects were observed in this review. Long-term, well-designed randomised controlled trials of recombinant growth hormone therapy in patients with cystic fibrosis are required prior to evaluation of human growth hormone treatment for routine use in patients.
Conflict of interest statement
Alexandra Haagenson declares that she has participated in marketing review studies on growth hormone (as well as other pharmaceutical) advertisements.
The remaining authors declare that there are no financial conflicts of interest and they do not have any associations with any parties who may have vested interests in the results of this review.
Figures


































































References
References to studies included in this review
-
- Hütler M, Schnabel D, Staab D, Tacke A, Wahn U, et al. Effect of growth hormone on exercise tolerance in children with cystic fibrosis. Medicine and Science in Sports and Exercise. 2002;34(4):567–572. [CFGD Register: GN125] - PubMed
-
- Schibler A, von der Heiden R, Birrer P, Mullis PE. Moderate improved exercise capacity in patients with cystic fibrosis after treatment with recombinant human growth hormone [abstract]. Proceedings of the 12th European Respiratory Society Annual Congress; 2002 Sept 14–18; Stockholm. 2002. p. P3287. [: GN121b]
-
- von der Heiden R, Kraemer R, Birrer P, Waldegg G, Mullis PE. Effect of growth hormone (r-hGH) treatment on working capacity, body composition, lung function and immunological parameters in patients with cystic fibrosis (CF) [abstract]. Proceedings of the 21st European Cystic Fibrosis Conference; 1997 June 1–6; Davos, Switzerland. 1997. p. 132. [: GN121a]
-
- Grasemann C, Ratjen F, Schnabel D, Reutershahn E, Vester U, Grasemann H. Effect of growth hormone therapy on nitric oxide formation in cystic fibrosis patients. European Respiratory Journal. 2008;31(4):815–821. [CFGD Register: GN127e] - PubMed
References to studies excluded from this review
-
- Alemzadeh R, Upchurch L, McCarthy V. Anabolic effects of growth hormone treatment in young children with cystic fibrosis. Journal of the American College of Nutrition. 1998;17(5):419–424. - PubMed
-
- Darmaun D, Hayes V, Schaeffer D, Welch S, Mauras N. Effects of glutamine and recombinant human growth hormone on protein metabolism in prepubertal children with cystic fibrosis. Journal of Clinical Endocrinology and Metabolism. 2004;89(3):1146–1152. [CFGD Register: GN90b] - PubMed
-
- Schaeffer D, Darmaun D, Punati J, Mauras N, Hayes VY. Use of glutamine and recombinant human growth hormone (RHGH) in children with cystic fibrosis [abstract] Pediatric Pulmonology. 2000;30(Suppl 20):323. [: GN90a]
-
- Eubanks V, Atchison J, Arani R, Clancy JP, Sorscher EJ, Wooldridge N, et al. Effects of megestrol acetate on energy intake, weight gain, body composition and resting energy expenditure in cystic fibrosis patients [abstract] Pediatric Pulmonology. 2000; 30(Suppl 20):322–33. [CFGD Register: GN86a; CRS–ID: 5500100000001740]
-
- Eubanks V, Koppersmith N, Wooldridge N, Clancy JP, Lyrene R, Arani RB, et al. Effects of megestrol acetate on weight gain, body composition, and pulmonary function in patients with cystic fibrosis. Journal of Pediatrics. 2002;140(4):439–444. [CFGD Register: GN86b; CRS–ID: 5500100000002066] - PubMed
References to studies awaiting assessment
-
- Bucuvalas JC, Chernausek SD, Alfaro MP, Krug S, Ritschel W, Wilmott RW. Insulin-like growth factor -I enhances linear growth in undernourished prepubertal children with cystic fibrosis [abstract] Pediatric Pulmonology. 1998;26(Suppl 17):355. [CFGD Register: GN123a; CRS–ID: 5500100000001298]
-
- Bucuvalas JC, Chernausek SD, Alfaro MP, Krug SK, Ritschel W, Wilmott RW. Effect of insulin-like growth factor-1 treatment in children with cystic fibrosis. Journal of Pediatric Gastroenterology and Nutrition. 2001;33(5):576–581. [CFGD Register: GN123b; CRS–ID: 5500100000002045] - PubMed
-
- Hardin DS, Ellis K, McConnell RA, Seilheimer DK. Growth hormone improves lean body mass in prepubertal CF children [abstract] Pediatric Pulmonology. 1998;26(Suppl 17):357. [CFGD Register: GN122a]
-
- Hardin DS, Ellis KJ, Dyson M, Rice J, McConnell R, Seilheimer DK. Growth hormone decreases protein catabolism in children with cystic fibrosis. Journal of Clinical Endocrinology and Metabolism. 2001;86(9):4424–4428. [CFGD Register: GN122d] - PubMed
-
- Hardin DS, Ellis KJ, Dyson M, Rice J, McConnell R, et al. Growth hormone improves clinical status in prepubertal children with cystic fibrosis: results of a randomized controlled trial. Journal of Pediatrics. 2001;139(5):636–642. [CFGD Register: GN122e] - PubMed
References to ongoing studies
-
- Phase II Study of Growth Hormone in Children With Cystic Fibrosis. Ongoing study. 2001
-
- A Study to Evaluate Nutropin AQ for the Treatment of Growth Restriction in Children With Cystic Fibrosis. Ongoing study. 2003
Additional references
-
- ACSM’s Guidelines for Exercise Testing and Prescription. 7th Edition. Baltimore: Lippincott, Williams, & Wilkins; 2006. American College of Sports Medicine.
-
- Assael BM, Casazza G, Iansa P, Volpi S, Milani S. Growth and long-term lung function in cystic fibrosis: a longitudinal study of patients diagnosed by neonatal screening. Pediatric Pulmonology. 2009;44(3):209–215. [PUBMED: 19230003] - PubMed
-
- Barkhouse LB, Fahey J, Gillespie CT, Cole DE. Quantitating the effect of cystic fibrosis on linear growth by mathematical modelling of longitudinal growth curves. Growth, Development, and Ageing. 1989;53(4):185–1890. [PUBMED: 2638347] - PubMed
-
- Beker LT, Russek-Cohen E, Fink RJ. Stature as a prognostic factor in cystic fibrosis survival. Journal of the American Dietetic Association. 2001;101(4):438–442. - PubMed
-
- Borowitz D, Baker RD, Stallings V. Consensus report on nutrition for pediatric patients with cystic fibrosis. Journal of Pediatric Gastroenterology and Nutrition. 2002;35(3):246–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical