

Tubercular retinal vasculitis
- PMID: 23737572
- PMCID: PMC3702819
- DOI: 10.1136/bcr-2013-008924
Tubercular retinal vasculitis
Abstract
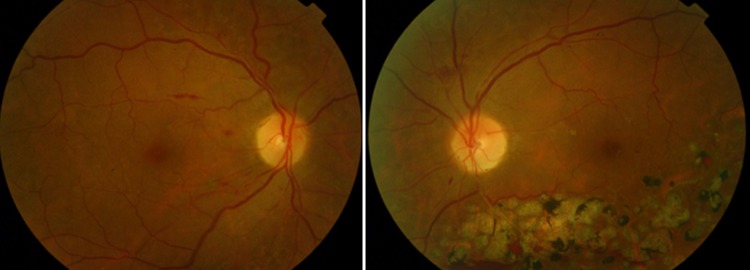
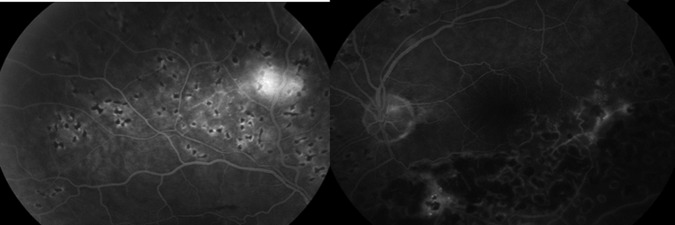
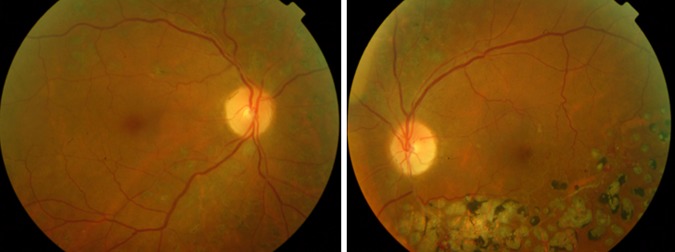
Intraocular tuberculosis (TB) infection can have different clinical manifestations including retinal vasculitis. It more frequently involves the veins and is associated with retina haemorrhages and neovascularisation. The diagnosis may be difficult and presumptive being based on clinical findings and evidence of systemic TB infection. The authors present a case of a 61-year-old woman with blurred vision and floaters in her left eye for 6 years, associated with recurrent vitreous haemorrahages. A temporal branch retinal vein occlusion was presumed. Four years later her right eye was also involved. Her best-corrected visual acuity (BCVA) was 20/50 in both eyes. Fundoscopic examination showed bilateral venous occlusion with vascular staining on fluorescein angiography suggestive of vasculitis secondary to Eales Disease (ED). The interferon gamma release assay (IGRA-QuantiFERON-TB Gold) was positive and antituberculosis treatment (ATT) was started. Her final BCVA was 20/20 bilaterally, without recurrences over a follow-up of 15 months. The use of ATT is likely to reduce recurrent vitreous haemorrhages and eliminate future recurrences.
Figures
References
-
- Alvarez S, McCabe WR. Extrapulmonary tuberculosis revisited: a review of experience at Boston City and other hospitals. Medicine (Baltimore) 1984;2013:25–55 - PubMed
-
- Kotake S, Kimura K, Yoshikawa K, et al. Polymerase chain reaction for the detection of Mycobacterium tuberculosis in ocular tuberculosis. Am J Ophthalmol 1994;2013:805–6 - PubMed
-
- Gupta V, Arora S, Gupta A, et al. Management of presumed intraocular tuberculosis: possible role of the polymerase chain reaction. Acta Ophthalmol Scand 1998;2013:679–8 - PubMed
-
- Bowyer JD, Gormley PD, Seth R, et al. Choroidal tuberculosis diagnosed by polymerase chain reaction. A clinicopathologic case report. Ophthalmology 1999;2013:290–4 - PubMed
-
- Barondes MJ, Sponsel WE, Stevens TS, et al. Tuberculous choroiditis diagnosed by chorioretinal endobiopsy. Am J Ophthalmol 1991;2013:460–1 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical